RSNA2019: Ultrafast brain MRI valid alternative to CT for emergent patients with non- traumatic neurological symptoms
A 5-minute protocol for noncontrast brain magnetic resonance imaging (MRI) may be a valid alternative to head computed tomography (CT) for emergency patients presenting with acute neurological symptoms, according to German researchers who presented at the 2019 RSNA annual meeting.
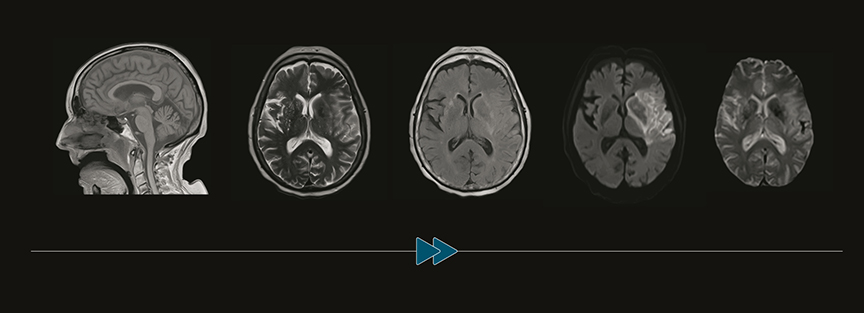
Image courtesy of Massachusetts General Hospital and Athinoula
A. Martinos Center for Biomedical Imaging.
Their study, conducted in Munich, Germany, demonstrated that ultrafast MRI identified more lesions than CT, and changed patient management in 10% of cases.
“Acute non-traumatic neurological symptoms are among the main reasons people go to the emergency department (ED), and represent 15% of the general emergency department population,” Philipp M. Kazmierczak, MD, of the Klinik und Poliklinik für Radiologie at the Klinikum der Universität München, told attendees at scientific session. “In most institutions, CT is the modality of choice because the examination is rapid, cost-efficient, and CT scanners are widely available.”
“However, MRI is the reference standard for detection and differential diagnosis of intracranial pathologies. But its use is limited due to long acquisition times for multi-sequence protocols. But through optimization of sequence parameters and the application of new parallel imaging technique, it is now possible to acquire a 5-sequence protocol (GOBrain, Siemens Healthineers) in less than 5 minutes,” he explained. The sequences and their acquisition time consisted of:
- T1 GRE sag (0.41 min)
- FLAIR ax (1:52 min
- DWU ax (0:38 min)
- T2 TSE ax 1:02 min)
- T2* ax (0:06 min)
The researchers’ prospective study tested two hypotheses: that image quality and diagnostic performance of the ultrafast-MRI scan for intracranial pathologies are non-inferior to the standard brain MRI protocol, and that ultrafast-MRI can change patient management compared to CT alone.
The study included all ED patients presenting with acute, nontraumatic neurological symptoms and/or suspected intracranial pathology between January and October 2018. Patients were excluded if their CT showed findings correlating with signs/symptoms, if intravenous thrombolysis/mechanical recanalization had already been initiated, or if they had contraindications to MRI and/or were in unstable condition.
Two hundred thirty-eight of 449 admitted patients underwent CT. CT adequately explained signs/symptoms in 40 patients, and additional imaging studies were excluded for 71 patients. The study cohort ultimately consisted of 69 patients with a negative noncontrast CT; reported signs/symptoms included vertigo (23), paresthesia (16), impaired vision (14), headache (14), and aphasia (13). Patients were equally divided by gender, and ranged in age from 22 to 91 years, mean of 61.
Patients whose CT did not show demonstrate findings correlating with signs/symptoms underwent MRI scanning with a 3 Tesla noncontrast scan with two protocols of five standard sequences. One was a standard-length protocol with a 15:11 acquisition time, and the other an ultrafast MRI with an acquisition time of 4:33. Two independent, blinded neuroradiologists analyzed the exams for quality using the 5-point Likert scale. They also calculated sensitivity and specificity for intracranial lesions.
Compared to CT alone, the neuroradiologists detected 93 additional lesions with the ultrafast MRI protocol and 101 with the standard MRI protocol. These pathologies included acute ischemia, edema, and hemorrhage/microbleeds. Eight lesions detected only by the standard MRI protocol included 5 microbleeds and 2 cases of acute ischemia. These did not cause any clinical consequences, as these patients also demonstrated at least one other ischemic lesion or microbleed.
“Image quality of ultrafast-MRI was equivalent to standard-length protocol, with excellent results for T2 sequences,” Dr. Kazmierczak said. “Ultrafast-MRI demonstrated high diagnostic accuracy, with a sensitivity of 94% and a specificity of 100%.”
MRI also had a direct impact on patient management. Based on MRI findings, patient management was changed in 6 patients; all were admitted to the stroke unit, and three had acetylsalicylic acid initiated.
“Our study [showed] that ultrafast-MRI is a valid alternative to CT in selected acute non-traumatic neurological emergency patients,” said Dr. Kazmierczak. “The ultrafast protocol can be extended according to suspected pathology, by adding brainstem-diffusion weighted imaging, contrast-enhanced T1, or cranial time-of-flight MR angiogram. In view of the missed findings, the use of standard-length DWI may be a reasonable protocol adjustment without significantly adding to the acquisition time,” concluded Dr. Kazmierczak.
This study was funded by Siemens Healthineers of Erlangen, Germany.
REFERENCE
- Kazmierczak P, Duhrsen M, Patzig M, et al. Diagnostic accuracy and impact on clinical patient management of an ultrafast 5 min/5 sequences brain MRI protocol in acute neurological emergencies. (SSE06-01). Radiological Society of North America 2019 Scientific Assembly and Annual Meeting, December 1-6, 2019, Chicago, IL. archive.rsna.org/2019/19018689.html. Accessed December 20, 2019.