Pyle-type metaphyseal dysplasia(2)
Images










Pyle-type metaphyseal dysplasia (or Pyle's disease)
Differential diagnosis: Chronic anemia (e.g. Sickle-cell disease), osteopetrosis, Gaucher disease and Niemann-Pick disease.
Findings
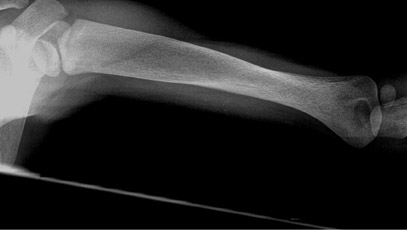
Skeletal survey revealed a mildly hyperostotic skull, with mild frontal bossing. There was metaphyseal widening of the long bones. Lateral bowing of the tibiae produced an S-shaped configuration (Figures 1C and 1D). However, the spine was normal (Figure 5).
Discussion
Pyle-type metaphyseal dysplasia is an extremely uncommon and rare genetic skeletal disorder inherited in an autosomal-recessive pattern (Gorlin et al. 1970.1 This means that both parents are unaffected, but there is a 25% chance the affected alleles will pass to a developing embryo and produce the widened biones. The actual gene or genetic defect is unknown, and cannot, therefore, be tested. The striking radiographic manifestations contrast with the relatively normal clinical features. Genu valgum is the only consistent abnormality.
Pyle first described the skeletal anomaly in 1931. Less than 35 genuine cases have since been reported.
Pyle-type metaphyseal dysplasia is clinically, radiographically and genetically distinct from craniometaphyseal dysplasia, a relatively common condition with which it has been confused. Pyle-type metaphyseal dysplasia must be distinguished and separated from craniometaphyseal dysplasia, for prognostication, since deafness, facial paralysis and occasional impairment of vision may result from cranial nerve compression in the latter, whereas, they are unusual in the former.1,2
Bone fragility and spinal malalignment or scoliosis is infrequent but are well-documented complications.3,4 Carious and misplaced teeth,4 and patchy sclerosis of the cranial vault with associated moderate supraorbital prominence and prognathism are features that have been reported in Pyle-type metaphyseal dysplasia.3
Genetic considerations are also relevant, as craniometaphyseal dysplasia is transmitted as an autosomal dominant, whereas, inheritance in Pyle-type metaphyseal dysplasia is autosomal recessive.5
In Pyle-type metaphyseal dysplasia there are gross abnormalities of the tubular bone modeling, with associated mild sclerosis of the cranium. Prominent radiographic features in the long tubular bones consist of splaying of the metaphyses with relative constriction of the diaphyses. The changes are most obvious in the distal femora, where the appearance has been likened to an "Erlenmeyer flask." Failure of modeling may also be seen in the short tubular bones, with widening of the medial ends of the clavicles, sternal ends of the ribs and pubic bones.
Conclusion
In spite of the striking radiographic manifestations, there are a few clinical stigmata and the condition has a benign course.
- Gorlin RJ, Koszalka MF, Spranger J. Pyle's disease (familial metaphyseal dysplasia. A presentation of two cases and argument for its separation from craniometaphysealdyslasia. J Bone Joint Surg Am. 1970;52(2):347-354.
- Mabille JP, Benoit JP, Castera D. Dysplasie metaphysaire de Pyle. Ann of Radiol (Paris). 1973;16:723-730.
- Pyle, E. A case of unusual bone development. J Bone Joint Surg Am. 1931;13:874-876.
- Bawkin, H, Krida, A. Familial metaphyseal dysplasia. American Journal of Diseases of Children. 1937;53:1521-1527.
- Raad MS, Beighton, P.Autosomal recessive inheritance of metaphyseal dysplasia (Pyle disease). Clin Genet. 1978;14: 251-256.