Prostate artery embolization
Images
This case is brought to you by Guerbet, LLC.
Case Summary
A 61-year-old man presented with a 15-year history of urinary symptoms secondary to benign prostatic hyperplasia (BPH). He had a known prostate size of 70 grams (normal 20-30 grams), and his chief complaint was hesitancy and intermittency of urination. Initially, he was treated with medications for his symptoms (tamsulosin and finasteride), but treatment was discontinued due to sexual side effects. After failure to improve using herbal/holistic supplements to relieve his symptoms, he found his symptoms were having a significant negative effect on his quality of life (QOL). However, he was wary of pursuing a surgical solution such as transurethral resection of the prostate (TURP), because of the potential side effects associated with the procedure. Instead, he decided to undergo prostatic artery embolization (PAE).
Diagnosis
Urinary symptoms secondary to BPH
Image Findings/Results
The patient underwent a PAE from a femoral artery approach (as he was too tall for a radial artery approach). To begin, a 5-Fr catheter was placed into his left internal iliac artery, and angiography demonstrated that his prostatic artery arose from the internal pudendal artery. (Note: the patient also had a history of bilateral hip arthroplasty, as is evident on the images.) Prior to embolization, an arterial anastomosis to the rectum was coil-embolized with a 3/2-mm Tornado® Embolization Coil (Cook Medical, Bloomington, IN, USA). Additionally, an arterial anastomosis to the internal pudendal artery was embolized with a similar coil.
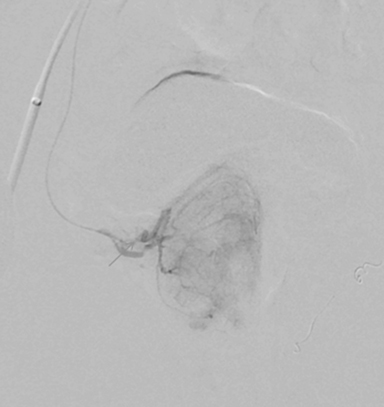
At that point, a 2.4-Fr SeQure® microcatheter (Guerbet, Roissy CdG, France) was inserted into the left prostatic artery, and the left hemi-prostate was embolized with 250 m Embozene™ Microspheres (Boston Scientific, Marlborough, MA, USA) until flow was sluggish, at which point, embolization was completed with a gel-foam slurry. When using the SeQure® catheter, the embolic solution can become more concentrated as the fluid component exits the holes within the distal catheter; therefore, we recommend the initial solution be adequately diluted to prevent aggregation and occlusion of the catheter. A Waltman loop maneuver was then used to select the right internal iliac artery with the 5-Fr catheter. Angiography was again performed, demonstrating the right prostatic artery arising from a vesico-prostatic trunk. The SeQure® microcatheter was then reinserted, and more selective angiography demonstrated the right hemi-prostatic blush (Figure 1). Embolization was performed with 250 m particles. When flow was once again sluggish, embolization was completed with the gel-foam slurry.
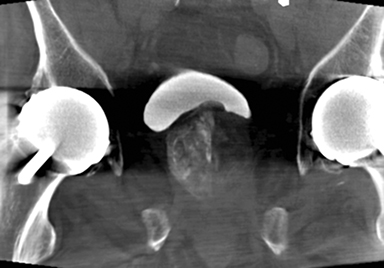
After the catheters were removed, a noncontrast, cone-beam, computed tomography (CT) examination demonstrated contrast retention throughout the prostate, suggesting complete embolization (Figure 2).
Discussion
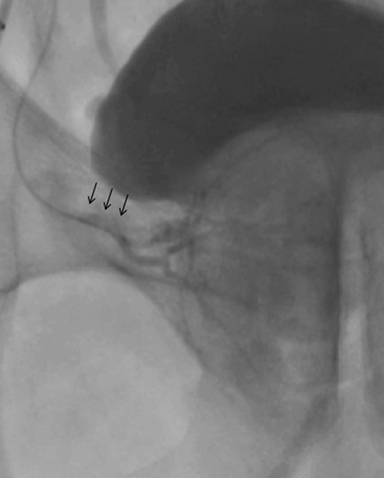
The SeQure® catheter was designed to reduce premature embolic reflux during embolization procedures. In this case, after initial embolization, contrast was observed exiting through the side hole at the distal segment of the catheter, creating the protective pressure gradient and preventing reflux (Figure 3). This potentially results in more particles being injected into the prostate compared to a standard end-hole catheter. The final cone-beam CT images suggest that this catheter is capable of thorough embolization of the prostate.
Importantly, the patient was evaluated before and after the procedure for symptom severity using the International Prostate Symptom Score (IPSS) questionnaire, an 8-question tool used to screen for, diagnose, and track symptoms of BPH. The IPSS has 7 questions related to symptoms and 1 related to QOL. In this case, the patient’s baseline IPSS was 25 (on a scale of 1 to 35; 25 is severely symptomatic) and his QOL was 4 (on a scale of 0 to 6; 4 is mostly dissatisfied). Three months’ post procedure, his IPSS score was 10 (low-to-moderately severe) and his QOL score was 1 (pleased), indicating that PAE performed with a SeQure® catheter successfully alleviated this patient’s symptoms.
Conclusion
PAE performed with a SeQure® catheter is an emerging interventional technique that can be used successfully to manage patients with urinary tract symptoms secondary to BPH.
Suggested Readings
- Gao YA, Huang Y, Zhang R, et al. Benign prostatic hyperplasia: prostatic arterial embolization versus transurethral resection of the prostate--a prospective, randomized, and controlled clinical trial. Radiology. 2014;270:920-928.
- Pisco JM, Bilhim T, Pinheiro LC, et al. Medium- and Long-Term Outcome of Prostate Artery Embolization for Patients with Benign Prostatic Hyperplasia: Results in 630 Patients. J Vasc Interv Radiol. 2016;27:1115-1122.
- Ray AF, Powell J, Speakman MJ, et al. Efficacy and safety of prostate artery embolization for benign prostatic hyperplasia: an observational study and propensity-matched comparison with transurethral resection of the prostate (the UK-ROPE study). BJU Int. 2018;122:270-282.
- Uflacker A, Haskal ZJ, Bilhim T, Patrie J, Huber T, Pisco JM. Meta-Analysis of Prostatic Artery Embolization for Benign Prostatic Hyperplasia. J Vasc Interv Radiol. 2016;27:1686-1697.
*The SeQure® microcatheter is not indicated or recommended for use with gel foam.
Citation
AJ I,. Prostate artery embolization. Appl Radiol. 2019;(4):38-39.
July 31, 2019