Pneumatosis Cystoides Intestinalis
Images


Case Summary
An elderly patient presented to the emergency department with a 48-hour history of diffuse abdominal pain and abdominal distension accompanied by an episode of vomiting. The patient had been chronically constipated but had no nausea, anorexia, diarrhea, or fever.
Previous medical history included congestive heart failure and atrial fibrillation, and no prior surgeries. Physical examination revealed mild diffuse abdominal pain with guarding. Laboratory tests were unremarkable, with normal white blood cell count, c-reactive protein and serum lactate.
Imaging Findings
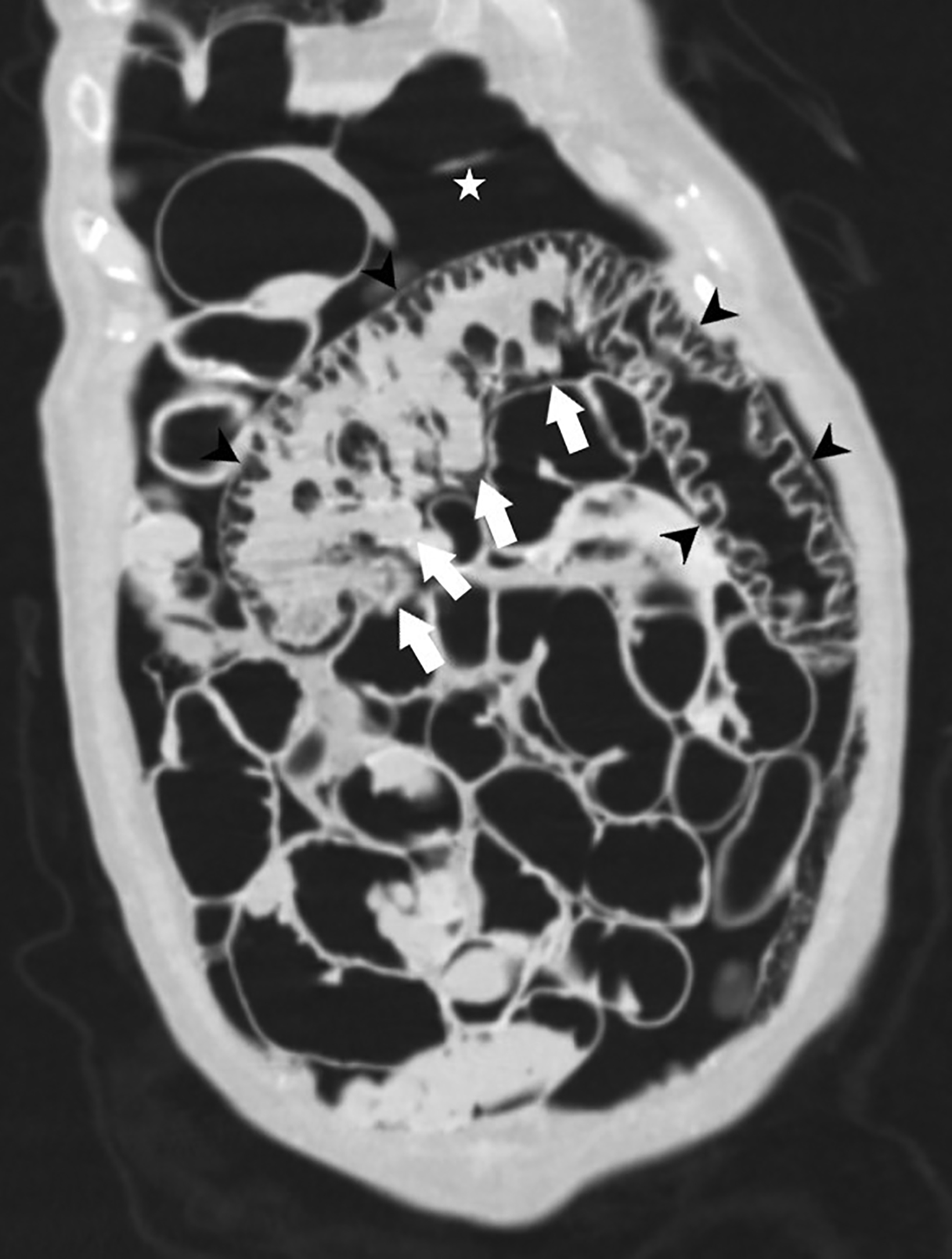
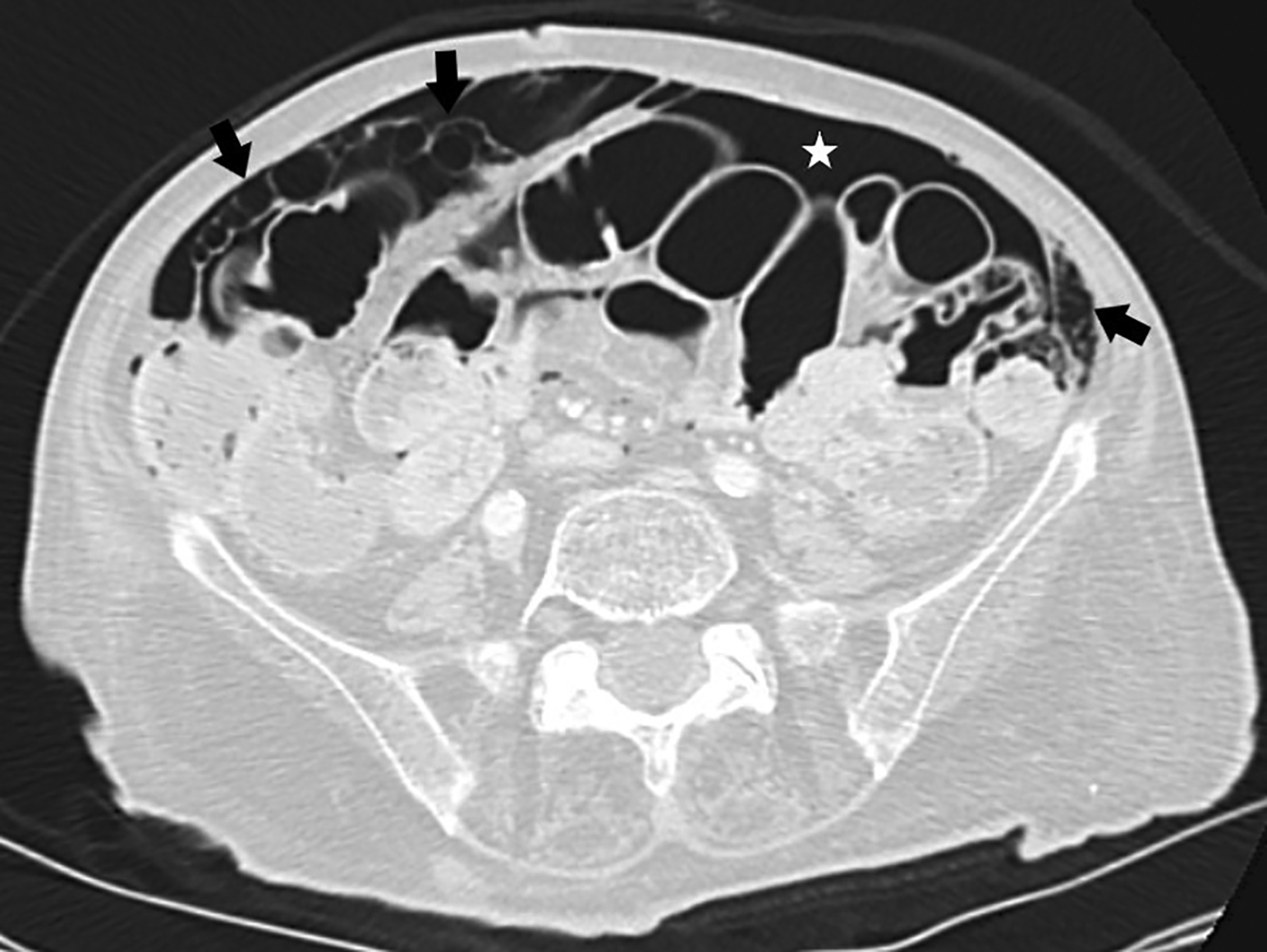
Abdominal radiography revealed a large-volume pneumoperitoneum, with mild distension of small bowel loops but no gas-fluid levels (Figure 1). A subsequent contrast-enhanced computed tomography (CT) scan demonstrated a large amount of free air and multiple cystic spaces within the wall of a segment of the jejunum and duodenum. There were also cystic spaces within the omentum and parietal peritoneal fascia, as well as several diverticula in the jejunum (Figure 2). There were no signs of bowel obstruction.
An emergency laparotomy revealed thickening of a jejunal segment with some diverticula associated with mesentery gas infiltration. No vascular compromise was found. Owing to suspicion of diverticular perforation, a segmental bowel resection was performed.
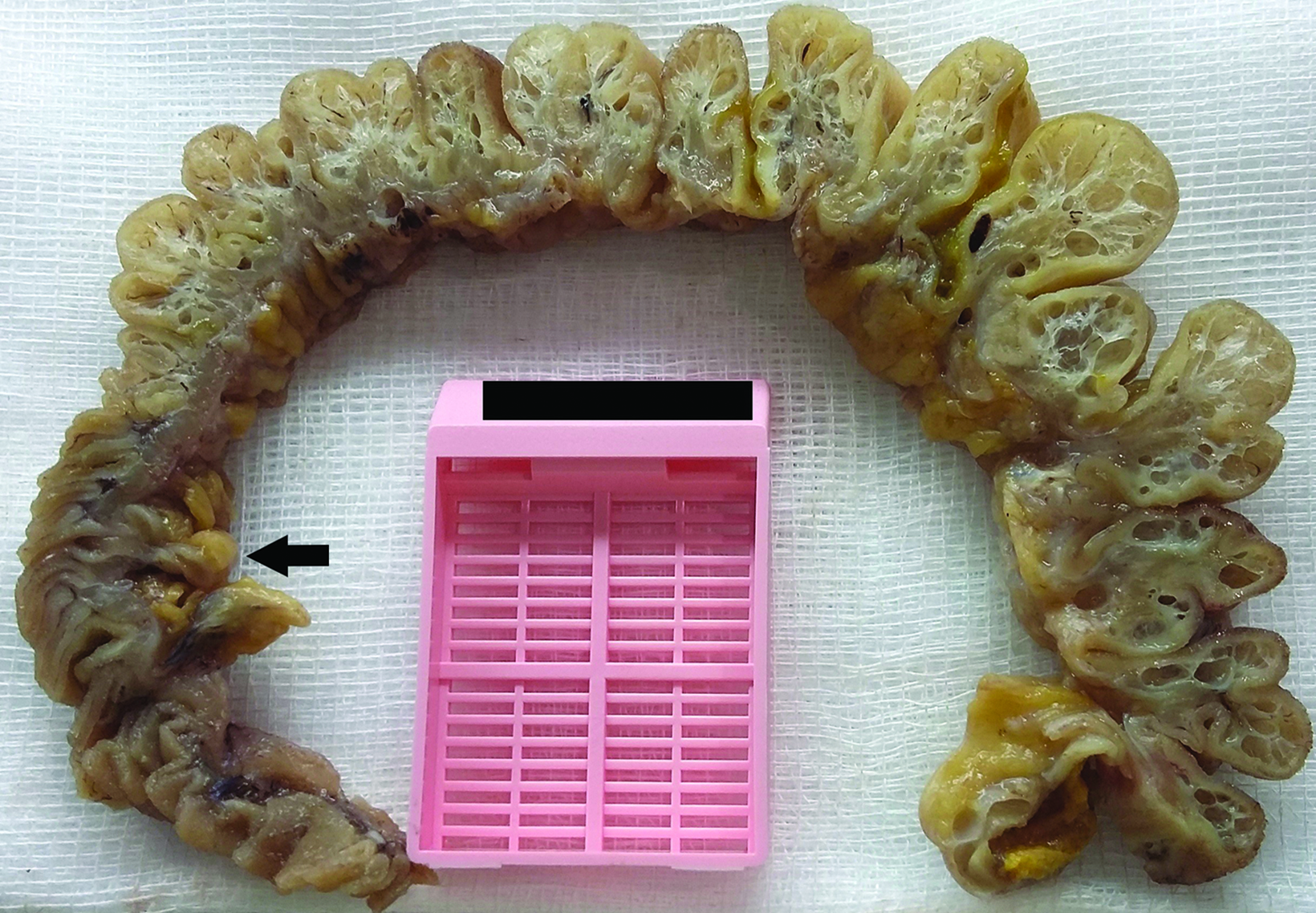
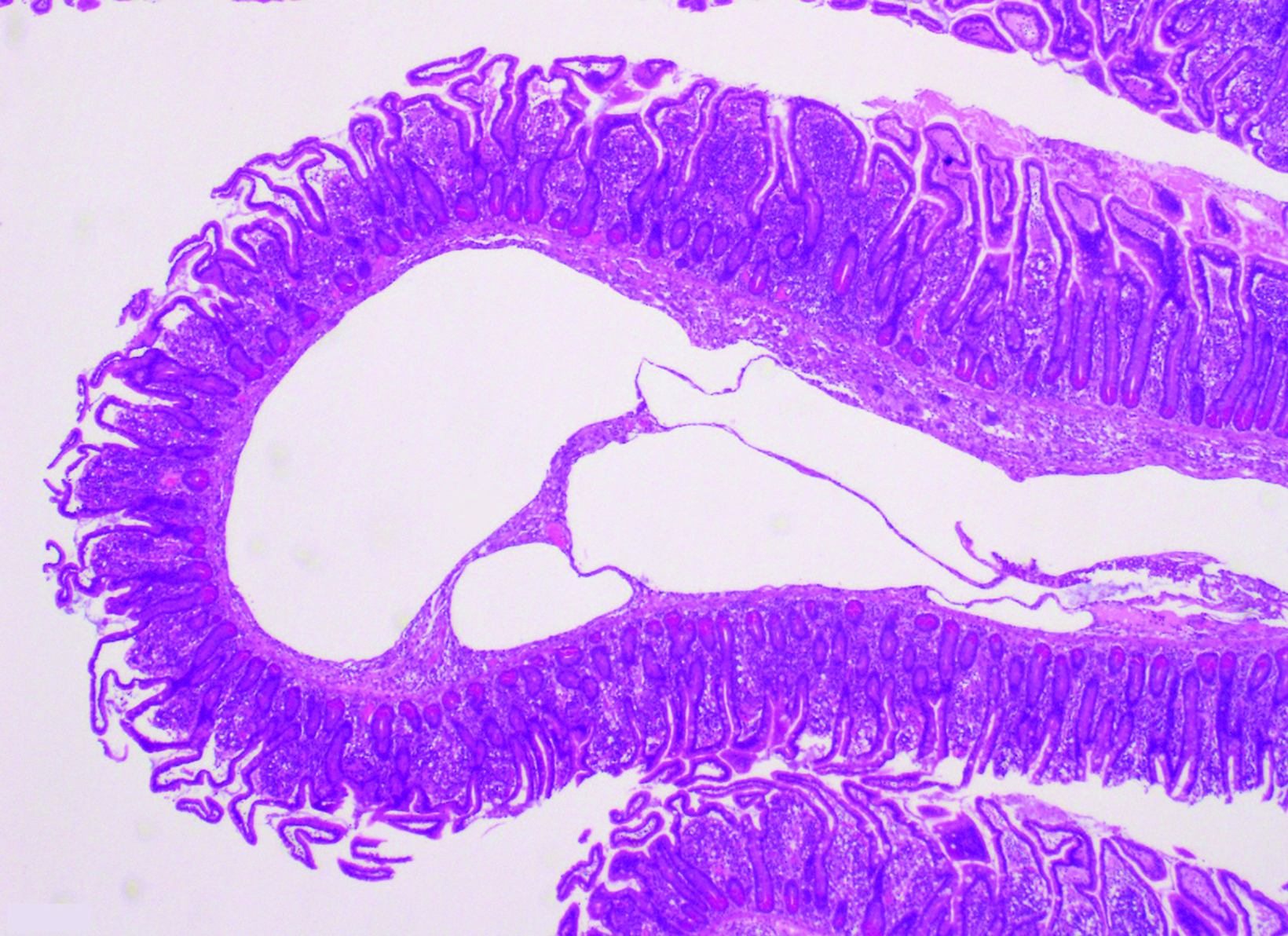
Pathology revealed multiple empty cysts expanding the submucosa, as well as in the subserosal layer with a sponge-like appearance, and some jejunal diverticula without signs of complication. Histological examination demonstrated several empty cysts predominantly in the submucosa but also in the mucosa, muscularis propria, and subserosa, which were lined by multinucleated giant cells (Figure 3).
Diagnosis
Pneumatosis cystoides intestinalis
Discussion
Pneumatosis intestinalis is a radiographic or physical finding characterized by the presence of gas within the wall of the intestine. Mesenteric ischemia and bowel obstruction represent the most life-threatening causes of pneumatosis intestinalis.1
A rare and benign subtype of intestinal pneumatosis, pneumatosis cystoides intestinalis (PCI) is characterized by multilocular, gas-filled cysts localized in the intestinal submucosa and subserosa. The condition can occur anywhere along the gastrointestinal tract, but the colon is the most common localization.2 Pneumatosis has been also found in unusual regions such as the mesentery, omentum, and hepatogastric ligament.3
Pneumatosis cystoides intestinalis can be divided into primary and secondary types. Causes of secondary PCI include pulmonary disease, inflammatory bowel disease, connective tissue disorders, iatrogenic procedures, certain medications, and organ transplantation.4 There are only a few case reports of pneumatosis intestinalis associated with jejunal diverticulosis.5,6 Zakhour and Clark suggested that the association of pneumatosis and diverticulosis could be related to mechanical and bacterial factors.6
Patients may be asymptomatic or they may demonstrate a broad spectrum of nonspecific gastrointestinal symptoms such as abdominal pain, distention and/or obstruction, as well as diarrhea, nausea, and vomiting.7
The imaging modalities most frequently used to diagnose pneumatosis intestinalis are radiography and CT, the latter of which is the most sensitive and specific for the condition. On radiography, PCI is characterized by radiolucency within the wall of the GI tract.4 Abdominal radiographic findings are detected in approximately two-thirds of patients.7 On CT, PCI appears as segmental or diffuse cystic spaces along the wall of the intestine; it can also appear in the mesentery and omentum. Visualization of CT images in lung windows helps to detect PCI.4
Two patterns of pneumatosis intestinalis have been described: a bubble-like or cystoid pattern characterized by separate bubbles of gas with a cystic appearance, and a linear pattern in which the gas has a curvilinear and a circumferential form in the bowel wall.1
The presence of linear pneumatosis and additional findings such as bowel-wall thickening, absent or intense mucosal enhancement, distended bowel, arterial or venous occlusion, ascites, large volume pneumoperitoneum, and portal or mesenteric venous gas increases the possibility of pneumatosis intestinal due to a life-threatening cause.7 Importantly, spontaneous small pneumoperitoneum can be associated with PCI, due to the rupture of subserosal cysts in the bowel wall.4
Histopathologic diagnosis of PCI is made in the presence of submucosal or subserosal empty spaces lined by multinucleated giant cells and macrophages.5
Pneumatosis cystoides intestinalis is often benign and only requires conservative treatment with antibiotics (especially metronidazole) and/or normobaric or hyperbaric oxygen therapy with follow-up. Surgical treatment should be considered for patients who remain symptomatic despite medical therapy or who develop PCI-related complications such as bowel obstruction, perforation, peritonitis, and necrosis.7
In our case, bowel resection was performed owing to the presence of a large amount of free peritoneal air and jejunal diverticula that raised the suspicion of perforation.
Conclusion
Owing to its rarity and nonspecific symptoms, PCI can be easily misdiagnosed. Correlating clinical history, imaging findings, and laboratory results is fundamental to differentiating benign from urgent cases and preventing misdiagnosis and inadequate treatment.
References
- Khalil PN, Huber-Wagner S, Ladurner R, Kleespies A, Siebeck M, Mutschler W, et al. Natural history, clinical pattern, and surgical considerations of pneumatosis intestinalis. Eur J Med Res. 2009;14:231-239. doi:10.1186/2047-783x-14-6-231.
- Wu LL, Yang YS, Dou Y, Liu QS. A systematic analysis of pneumatosis cystoids intestinalis. World J Gastroenterol. 2013;19(30):4973-4978. doi:10.3748/ wjg.v19.i30.4973.
- Wang Y, Wang Y, Zheng Y, Jiang H, Zhang J. Pneumatosis cystoides intestinalis: six case reports and a review of the literature. BMC Gastroenterology. 2018;18:100. doi:10.1186/s12876-018-0794-y.
- Ho LM, Paulson EK, Thompson WM. Pneumatosis intestinalis in the adult: benign to life-threatening causes. AJR Am J Roentgenol. 2007;188(6):1604-1613. doi:10.2214/AJR.06.1309.
- Sammon AM, Malcolm AJ. Pneumatosis cystoides intestinalis secondary to chronic jejunal diverticulitis. Postgrad Med J. 1979;55(649):820-821. doi:10.1136/ pgmj.55.649.820.
- Zakhour HD, Clark RG. Intramural gas cysts in a case of diverticular disease of the jejunum. Histopathology. 1982;6(3):363-369. doi:10.1111/j.1365-559.1982.tb02730.x.
- Sugihara Y, Harada K, Ogawa H, Otsuka F, Okada H. Pneumatosis cystoides intestinalis. J Lung Health Dis. 2018;2:24-7. doi: 10.29245/2689-999X/2017/1.1121.
References
Citation
AMC A, D S, RM M,. Pneumatosis Cystoides Intestinalis. Appl Radiol. 2022;(4):42-44.
July 13, 2022