Non-traditional thoracic duct embolization using an Angio-CT system
Images

Thoracic duct embolization is used in the treatment of chylothorax and is a minimally invasive alternative to thoracic duct ligation. The procedure is a 3-step process, which includes lymphangiography followed by catheterization of the cisterna chyli and then embolization of the thoracic duct closest to the leak or occlusion.1 Traditionally, lymphangiography has been the most time-consuming or rate-limiting aspect of the procedure. However, with the advent of newer technologies like 4D-CT (Angio-CT), this part of the procedure has the potential to be considerably shorter.
This article will outline the use of Angio-CT to perform thoracic duct embolization with direct CT-guided cisterna chyli (CC) puncture. We will additionally discuss other novel techniques involving thoracic duct embolization.
CASE PRESENTATION
A 57-year-old male underwent partial glossectomy and bilateral neck dissection for squamous cell carcinoma of the tongue. A surgical drain had to be placed in the left neck due to a chylous leak during the surgery. Postoperatively, chylous output remained high at more than 1000 mL/day for 10 days, and triglycerides were elevated at 285 mg/dL.
The decision was made to perform a thoracic duct embolization using Angio-CT (Infinix‑I 4D CT, Canon Medical Systems USA, Inc., Tustin, CA) and under conscious sedation and local anesthesia. Because Angio-CT allows for the use of CT and fluoroscopy in a single unit, a plan involving direct access to the cisterna chyli (CC) without lymphangiography, followed by fluoroscopic access into the thoracic duct was created. Access to two inguinal nodes with ethiodized oil was also performed in order to perform conventional lymphangiography in the event direct CC puncture failed.
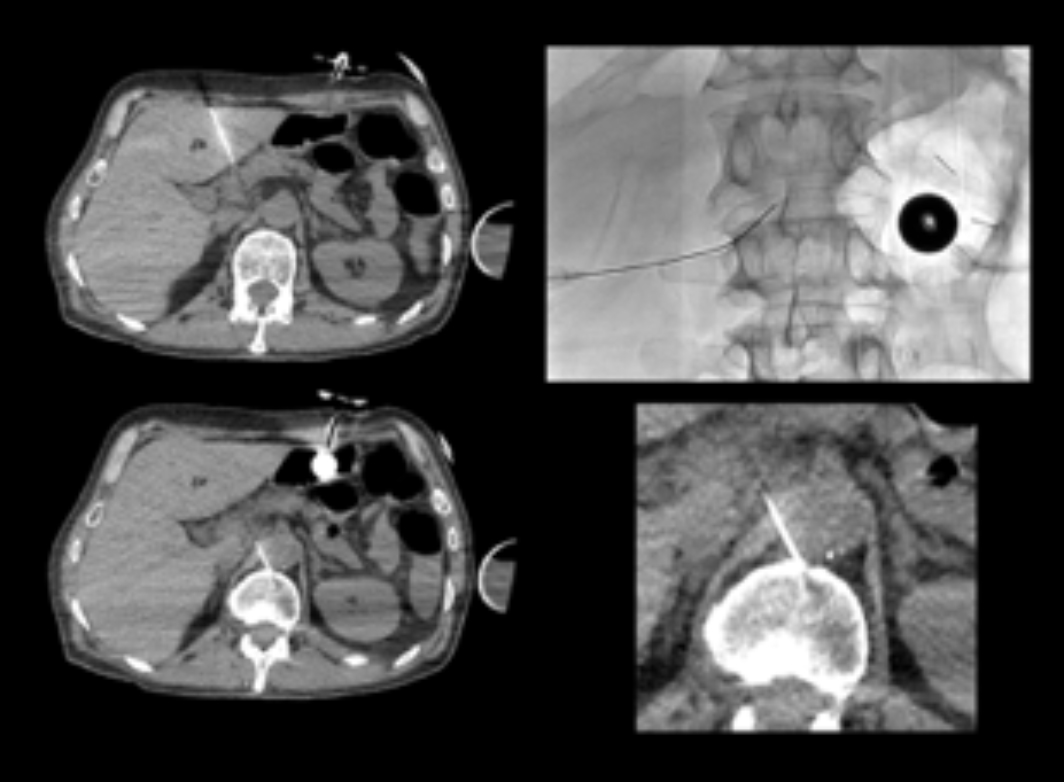
To identify the CC posterior to the aorta and anterior to the L1 vertebral body, a diagnostic CT of the abdomen was performed. Under CT guidance, a 22-G needle was punctured through and through the CC (Seldinger technique) (Figure 1). The needle was slowly withdrawn while injecting contrast to confirm appropriate placement in the CC using fluoroscopy. A 0.018” wire (GT® wire, Terumo Interventional Systems, Somerset, NJ) was then advanced through the needle and placed within the thoracic duct. The needle was then exchanged for a 0.018” Quick-Cross catheter (Philips Healthcare, Andover, MA).
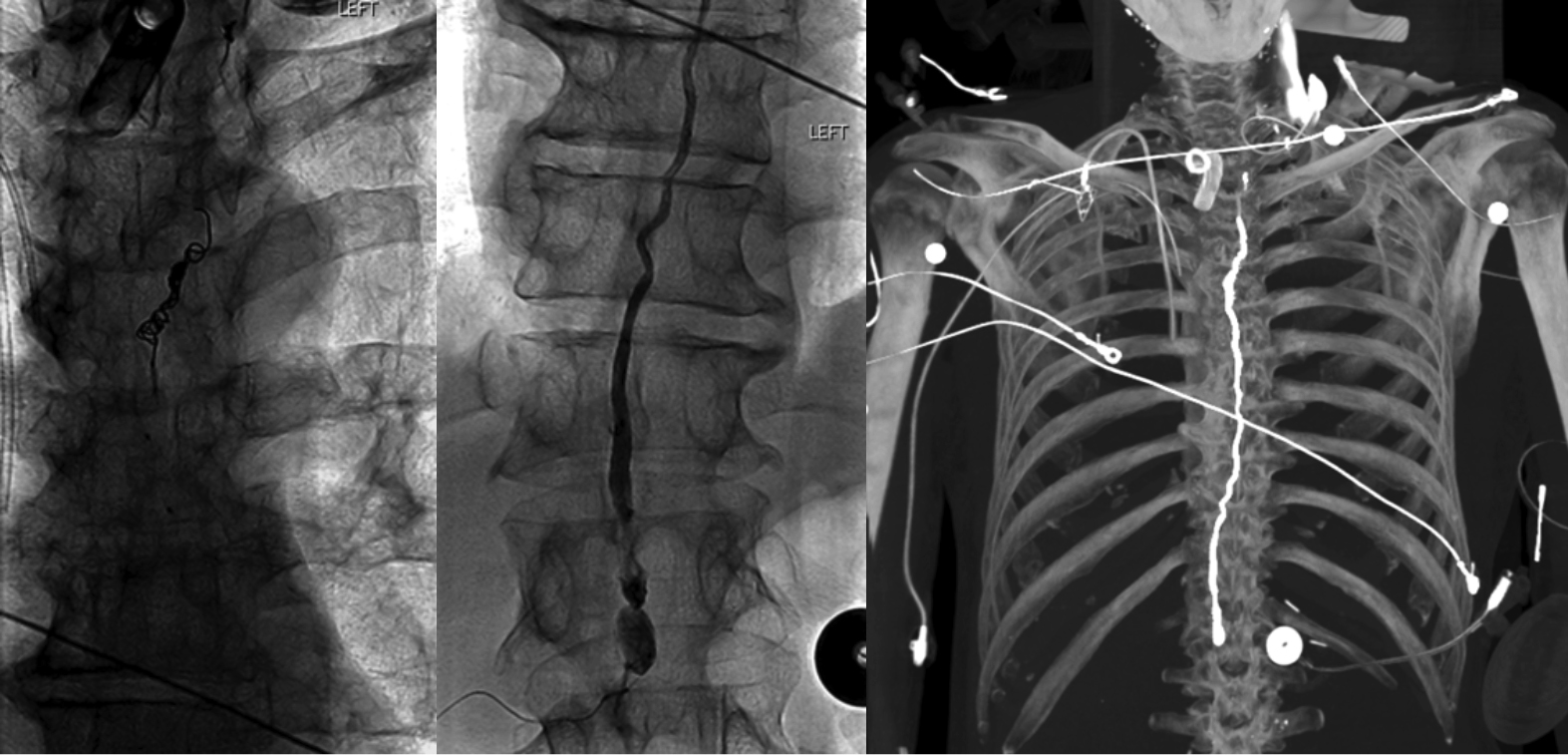
Next, ascending lymphangiography was performed to detect the location of the chyle leak (Figure 2). Using a combination of one 4 mm and five 6 mm pushable coils (Nester coils, Cook, Bloomington, Indiana), as well as ethylene-vinyl alcohol copolymer, the thoracic duct was embolized (Figure 3). A confirmatory CT was then performed upon completion to ensure treatment success and absence of complications. Prior to the completion of the procedure, spot radiographs confirmed that the ethiodized oil that was injected into the inguinal lymph nodes had only progressed into the pelvis. Total procedure time was 125 minutes including 18 minutes of fluoroscopy and air kerma of 252.6 mGy. There were no postprocedural adverse events the patient’s cervical drain output decreased to <30 mL/day.
In the present case, the use of Angio-CT allowed for a more streamlined approach in pursuing the thoracic duct embolization without the use of traditional lymphangiography and ethiodized oil. Alternative methods that have been described to mitigate postoperative lymphatic leak include approaching the leak through retrograde transcervical access, endovenous subclavian access, as well as injecting the leak with contrast and cannulating the thoracic duct using fluoroscopy.2,3,4 While these techniques are suitable alternatives to traditional techniques, they are often difficult to replicate and require technical expertise.4 The use of Angio-CT, therefore, is a useful because it can improve efficiency in a way that can be replicated on many levels.
REFERENCES
- Higgins M, Park AW, Angle JF. Chylothorax: Percutaneous 3mbolization of the thoracic duct. Operative Techniques in Thoracic and Cardiovascular Surgery. 2015;20(4):402-412.
- Koike Y, Hirai C, Nishimura J, Moriya N, Katsumata Y. Percutaneous transvenous embolization of the thoracic duct in the treatment of chylothorax in two patients. J Vasc Interv Radiol. 2013;24(1):135-137.
- Chung A, Gill AE, Rahman FN, Hawkins CM. Retrograde thoracic duct embolization in a pediatric patient with total cavopulmonary connection and plastic bronchitis. J Vasc Interv Radiol. 2015;26(11):1743-1746.
- Guevara CJ, Rialon KL, Ramaswamy RS, Kim SK, Darcy MD. US-Guided, direct puncture retrograde thoracic duct access, lymphangiography, and embolization: feasibility and efficacy. J Vasc Interv Radiol. 2016;27(12):1890-1896.