Non-neoplastic Cystic Lesions of the Central Nervous System, Part 2: Idiopathic and Acquired Cysts
Images
SA-CME credits are available for this article here.
Editor’s note: This is the second part of a two-part series. The first part appeared in the July/August 2022 issue of Applied Radiology.
A variety of developmental and acquired intracranial cysts are frequently encountered on imaging. Knowledge of their characteristics, localization and clinical behavior helps narrow the differential diagnoses.
In the first part of this series, we reviewed non-neoplastic, developmental cystic lesions, including prominent perivascular/Virchow-Robin spaces, epidermoid, dermoid, colloid, arachnoid, and Rathke cleft cysts. Epidemiologic and pathophysiologic features, clinical presentation, diagnosis, and radiologic characteristics for each were also discussed.
In this second part, we discuss various non-neoplastic idiopathic cystic lesions, including pineal, glioependymal, choroidal fissure and choroid plexus cysts, as well as acquired cystic lesions such as porencephalic and post-traumatic cysts. Each cystic lesion is discussed in terms of epidemiologic and pathophysiologic features, clinical presentation, diagnosis, and radiologic characteristics.
Idiopathic Cysts
Pineal Cyst
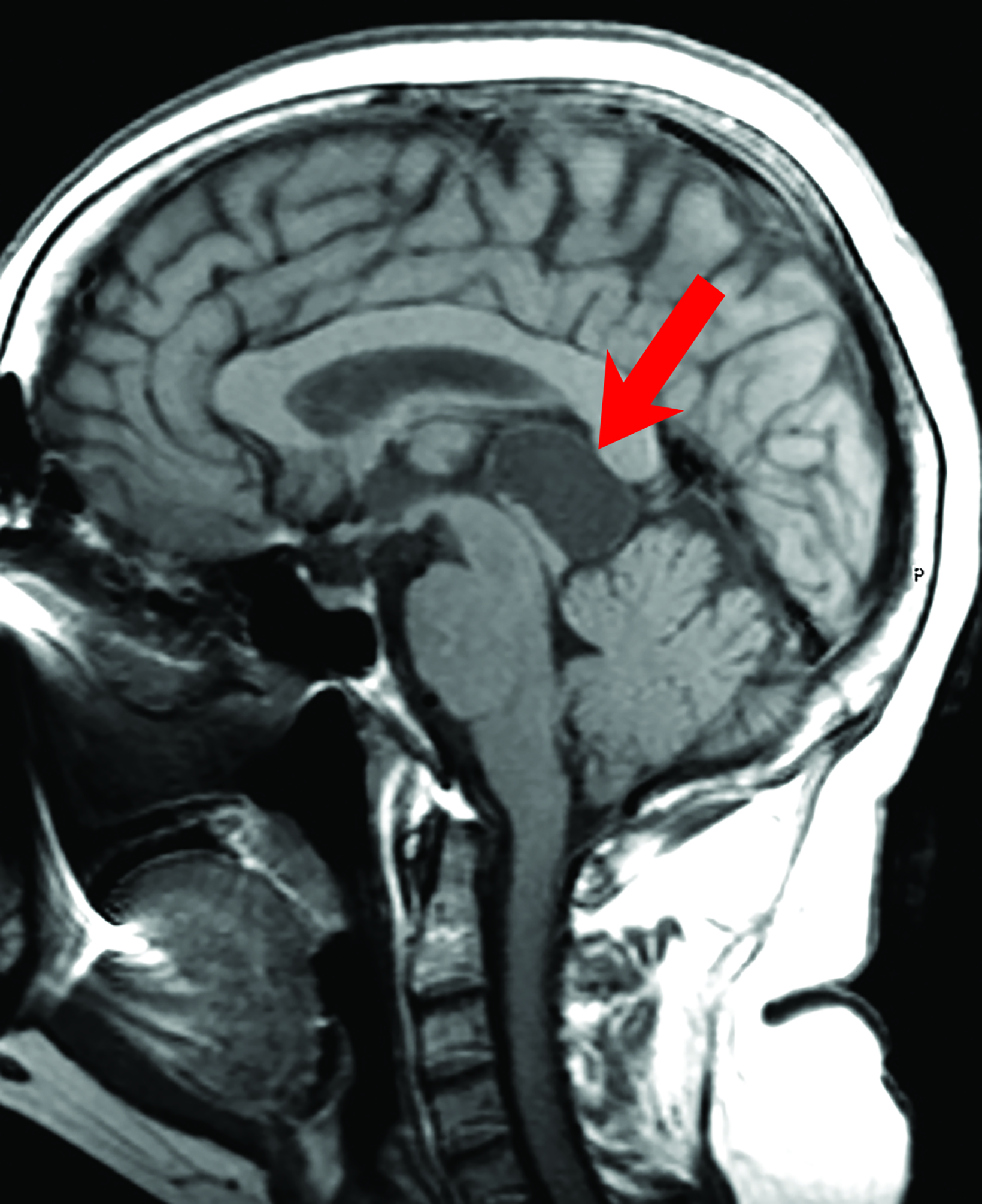
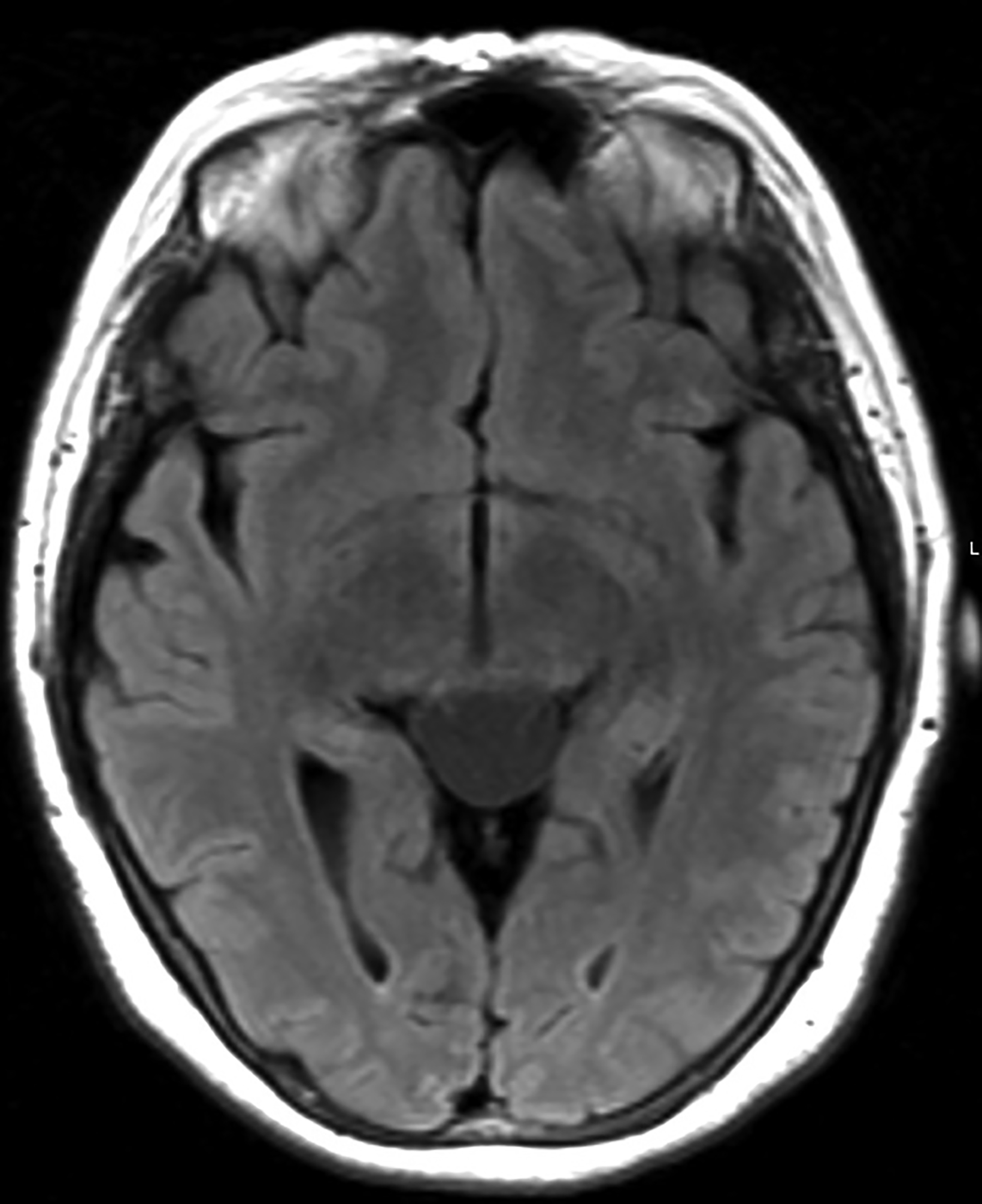
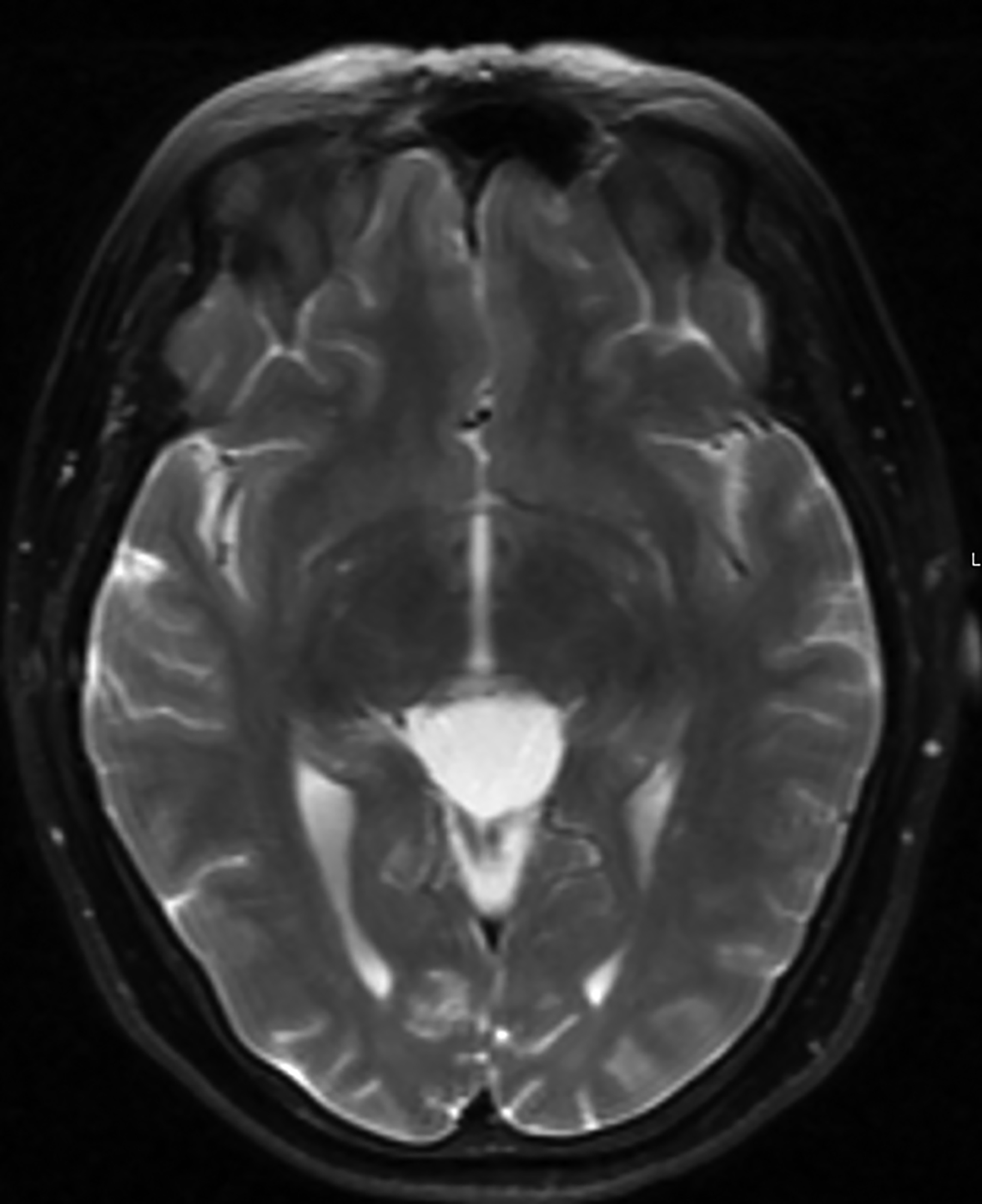
Pineal cysts are common but poorly understood. The prevailing theory is that cystic degeneration of the pineal gland is the etiology that explains the presence of residual pineal parenchyma in the cyst.1 These cysts are found in 10-20% of routine imaging cases.1,2 Pineal cysts may be seen in patients of any age, but most are identified in young adults.2 About 80% of pineal cysts are smaller than 1 cm and asymptomatic. Cysts larger than 1.5 cm may present with headache; in rare cases visual disturbances may occur as these cysts compress the tectum and cerebral aqueduct, resulting in Parinaud syndrome with obstructive hydrocephalus (Figure 1).2 Acute hemorrhage into a pineal cyst (pineal apoplexy) is also rare and may present with sudden headache, an abrupt change in mental status, and death.
Histologically, pineal cysts are lined with an outer fibrous connective tissue layer, a middle pineal parenchymal tissue layer with or without calcification, and an inner glial tissue layer.
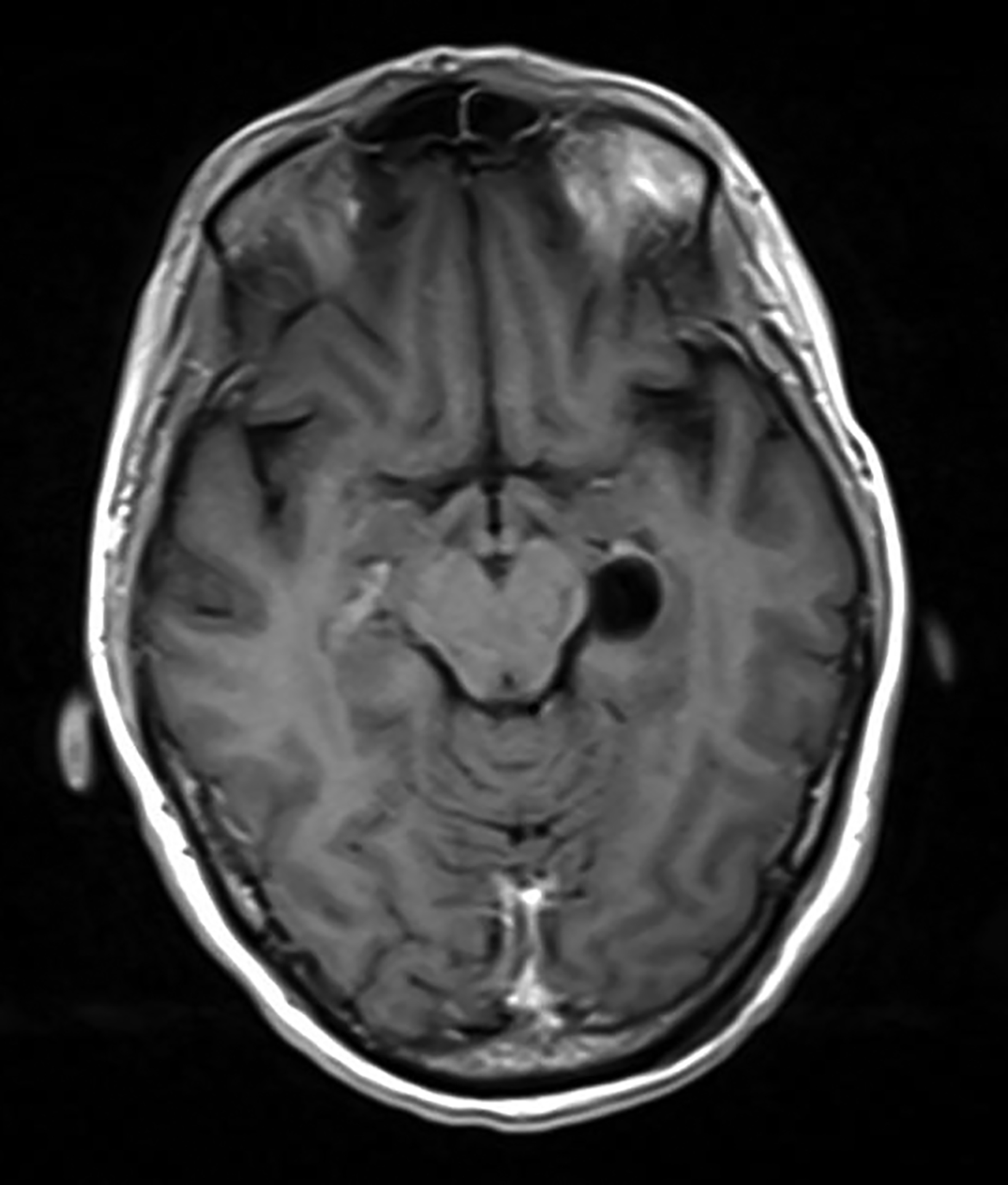
On computed tomography (CT), pineal cysts are isodense or slightly hyperdense to cerebrospinal fluid (CSF). On magnetic resonance images (MRIs), cysts are well-circumscribed round or oval, thin-walled, and lack mural nodularity or a soft-tissue component.
Pineal cysts have isointense or slightly hyperintense T1 signal as compared to CSF (Figure 1), and they are usually hyperintense on T2 sequences. Incomplete ing of the signal on fluid attenuated inversion recovery (FLAIR) sequences could be attributed to highly proteinaceous material.3 They usually show facilitated diffusion and are without hemorrhage. Curvilinear enhancement in the wall is related to remaining, surrounding normal pineal parenchyma.3
Glioependymal Cysts
Also known as neuroglial cysts, glioependymal cysts are rare intracranial cystic lesions that account for fewer than 1% of intracranial cysts. They may arise in various locations, most commonly intraparenchymal, followed by the subarachnoid space and intraventricular.4,5 The most frequent location of glioependymal cysts is in the periventricular white matter of the frontal lobe.
When they are large, glioependymal cysts may compress the adjacent brain parenchyma or obstruct the ventricles. Symptoms and signs may include headache, dizziness, motor deficit, seizures, hemifacial spasms, and coma.6 There is no gender predilection. Most cysts present during the first and third decades of life.6
Glioependymal cysts are typically hypodense on CT and isointense to CSF on all MRI sequences. There is typically no enhancement in the wall (Figure 2). Robles, et al, suggested lack of adjacent bone thinning may differentiate these cysts from arachnoid cysts.6 Definitive diagnosis can only be made on histopathology. The cysts are lined with a thin inner-ependymal layer, an intermediate glial layer, and an outer connective tissue layer.
Multiple names have been used to describe these cysts in the literature. They include neuroglial, ependymal, supratentorial, epithelial, and neuroepithelial cysts.6,7 Owing to the lesions’ unique wall structure, glioependymal cyst remains the preferred name.8
Choroidal Fissure Cyst
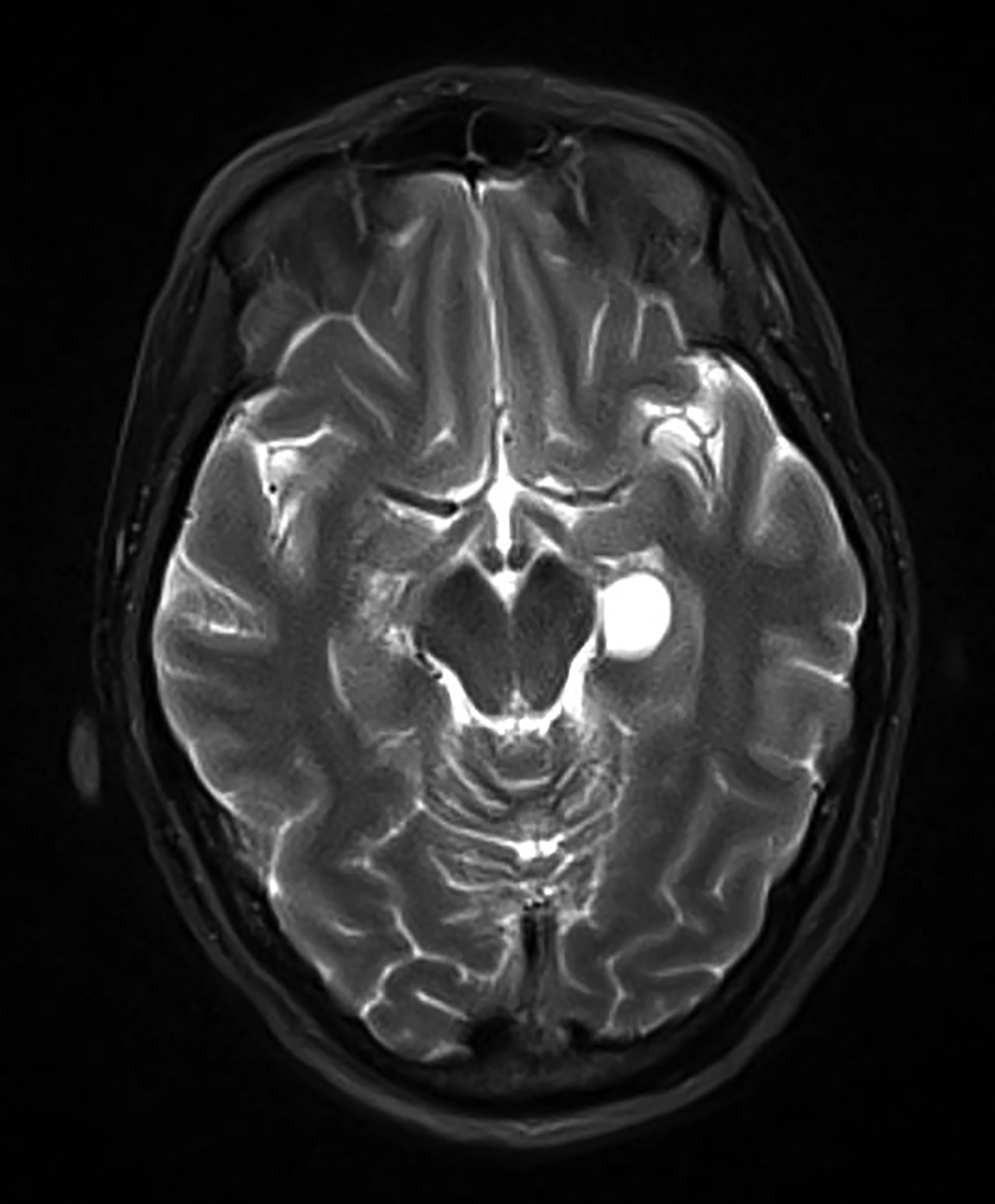
Choroidal fissure cysts are common, small (<30mm) intracranial cysts centered in the choroidal fissure along the mesial temporal lobe. The choroidal fissure is a cleft that contains the choroid plexus of the inferior horn of the lateral ventricle and extends from the hippocampal fissure in the anterior temporal lobe to the atrium of the lateral ventricle at the level of the foramen of Monro.9
The separation between the temporal horn and the choroidal fissure is formed by the tela choroidea, epithelially derived from the roof plate of the telencephalon. Formation of an ependymal diverticulum, which subsequently becomes isolated from the ventricular system and its vascular pia mater, results in a choroidal fissure cyst.10
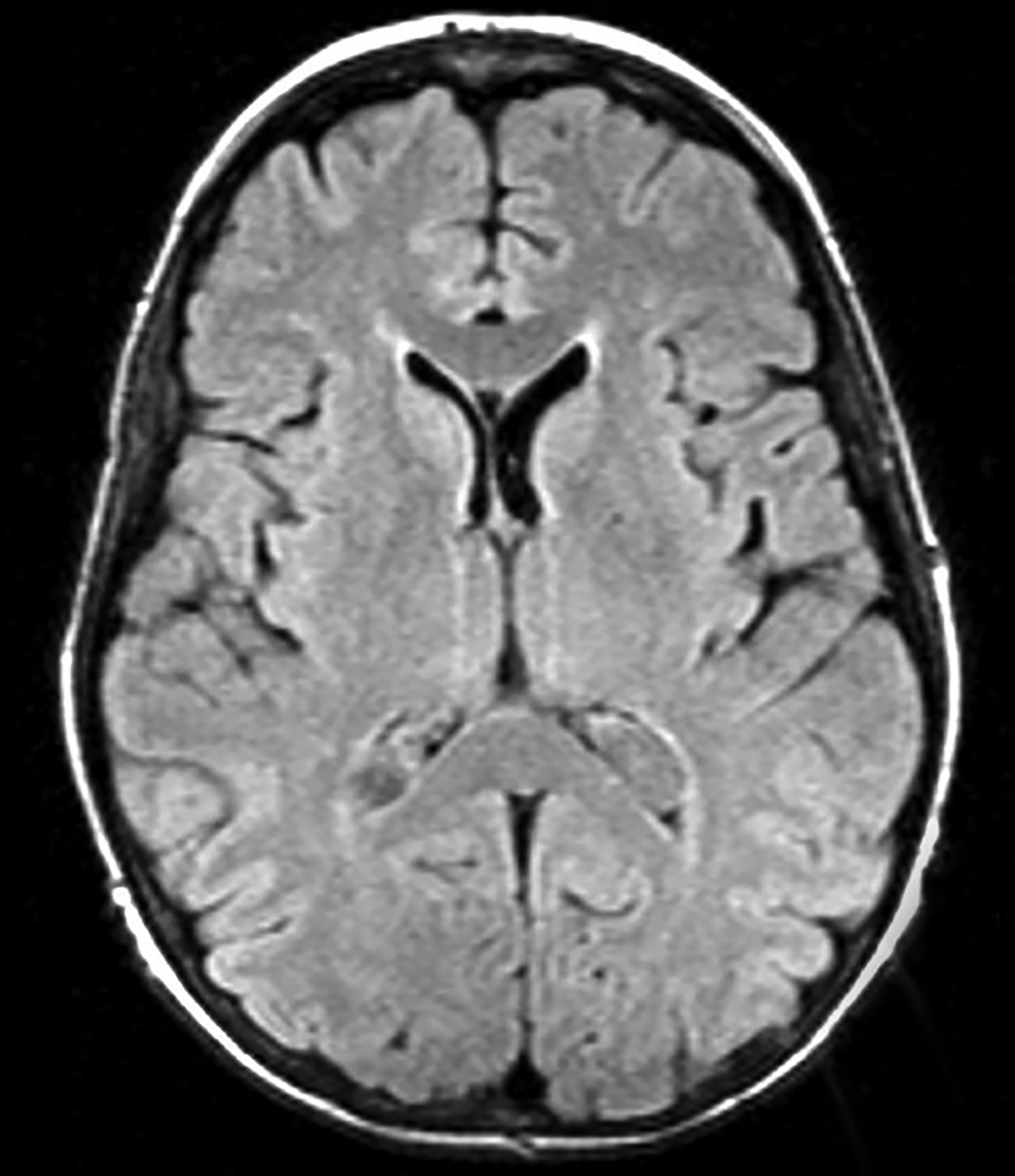
Choroidal fissure cysts tend to be oval, with their long axes parallel to the choroidal fissure in the anteroposterior plane.10 These cysts rarely enlarge; however, when they do, headaches, epilepsy, tremor, paresthesia, hemiparesis, gait disturbance, vertigo, or hearing loss may result.10 On imaging, choroidal fissure cysts are isodense to CSF on CT and isointense to CSF on all MRI sequences (Figure 3). There should be no contrast enhancement or diffusion restriction.11,12 Karatas, et al, reported a rare occurrence of intra-cystic hemorrhage within a choroidal fissure cyst and suggested the presence of heterotopic choroid plexus tissue as the source of the bleeding.13
Differentiating temporal horn enlargement resulting from focal temporal lobe atrophy or mesial temporal sclerosis from a choroidal fissure cyst is imperative.10 The correct diagnosis can be determined by the pattern of choroid plexus displacement. In the case of a choroidal fissure cyst, the choroid plexus is displaced laterally, whereas in temporal horn enlargement the choroid plexus is displaced medially. Truly distinguishing between choroidal fissure and glioependymal cysts can only be made on histopathology.12
Choroid Plexus Cyst
Choroid plexus cysts are very common in adults. They are usually bilateral and their incidence increases with age. Choroid plexus cysts in early life are most often incidental and inconsequential, unlike “syndromic” choroid plexus cysts.14 On rare occasions choroid plexus cysts may enlarge and obstruct the ventricles. Syndromic choroid plexus cysts are encountered in 1% of pregnancies and typically seen in the third trimester. They may be associated with Trisomy 18 or 21 and rarely cause hydrocephalus.
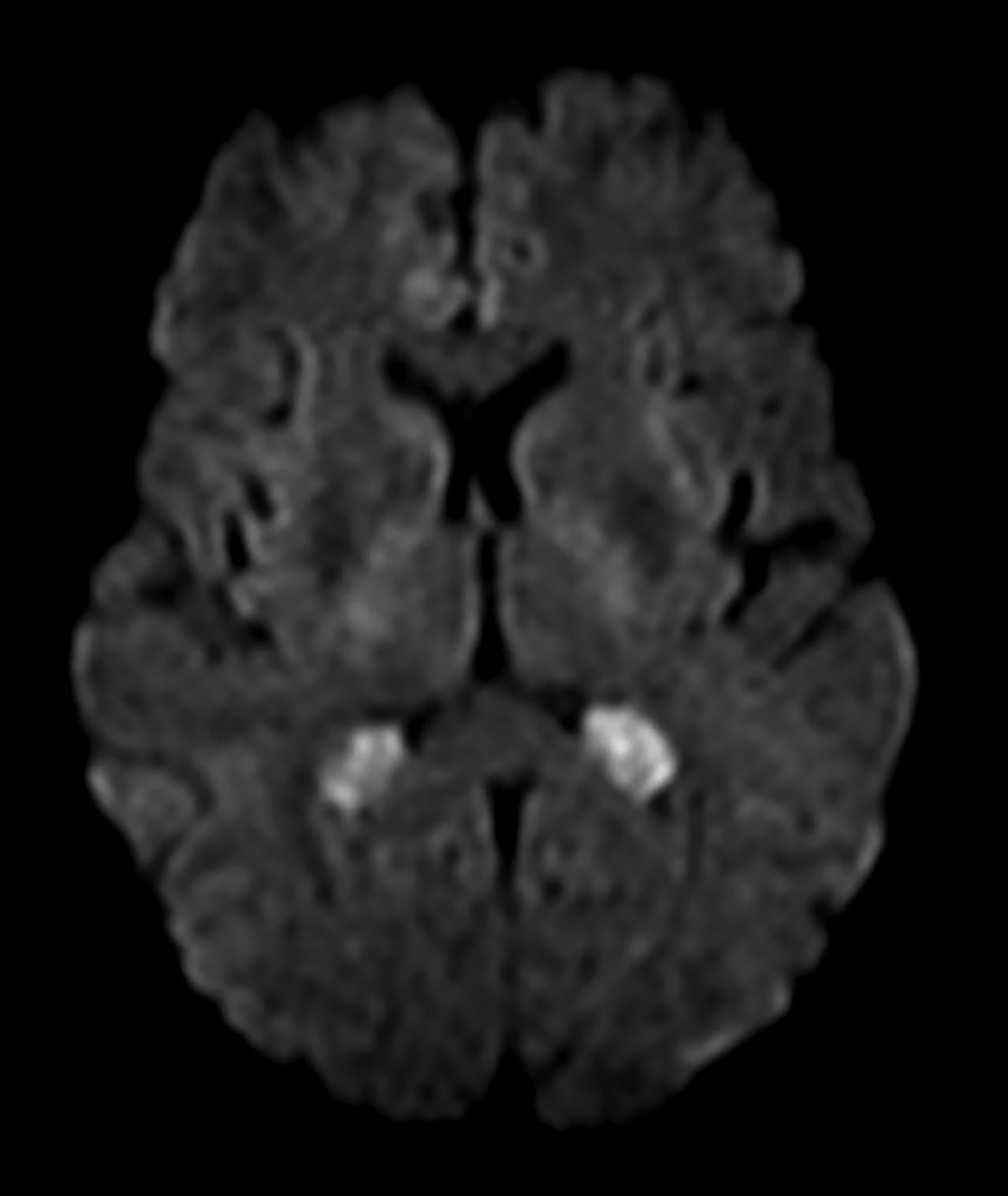
On CT, choroid plexus cysts are isodense or slightly hyperdense to CSF and surrounded by the choroid plexus. On MRI, they commonly demonstrate diffusion restriction (65%) with variable signal on T1 and T2 weighted sequences (Figure 4). Enhancement in the periphery of the cyst is related to the native vascular tissue of the choroid plexus draped over the cyst.14 Most cysts are smaller than 2 cm in diameter, not associated with hydrocephalus, and require no medical attention. Larger cysts may result in hydrocephalus requiring shunting or other surgical intervention.
Acquired Cysts
Porencephalic Cyst
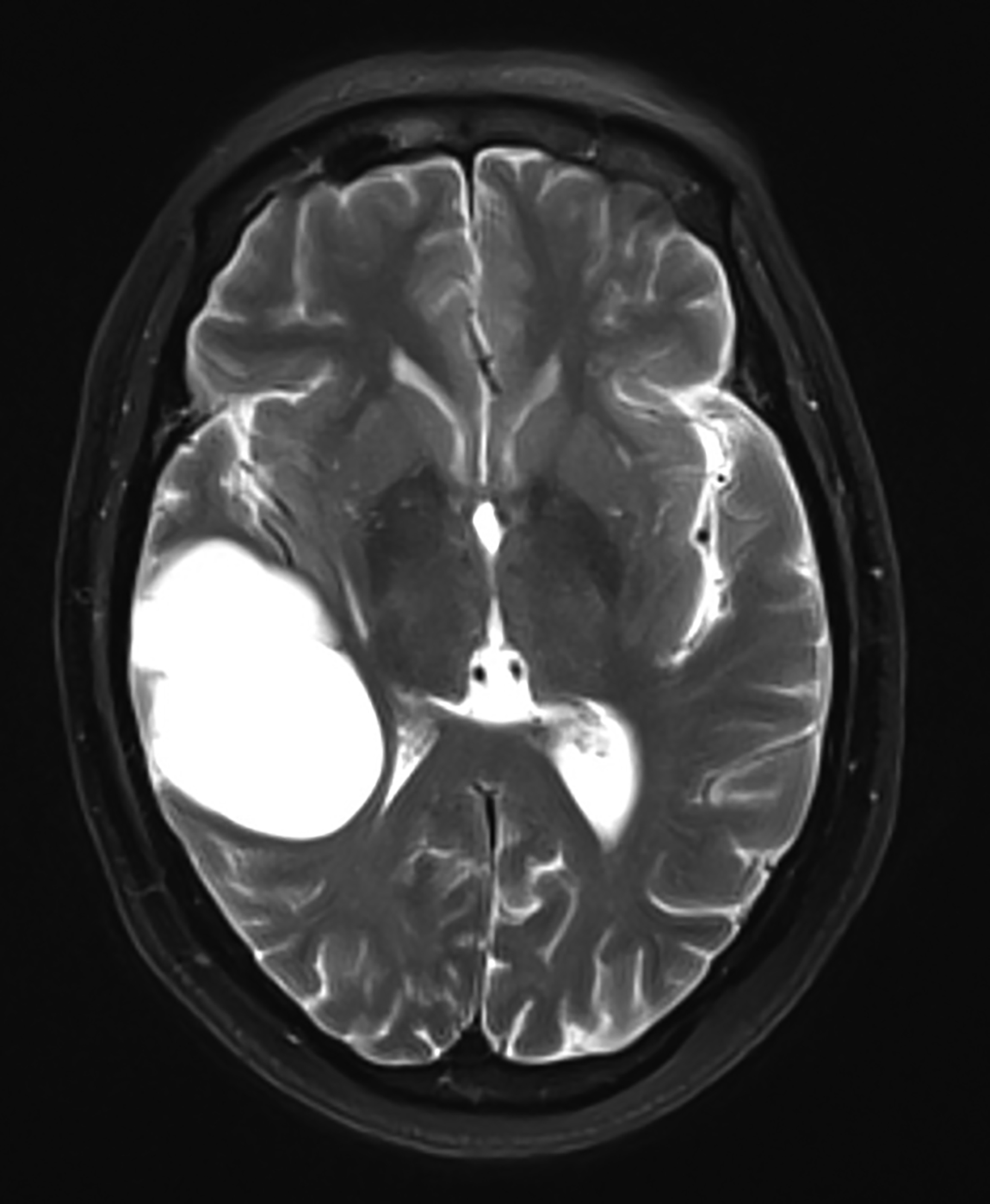
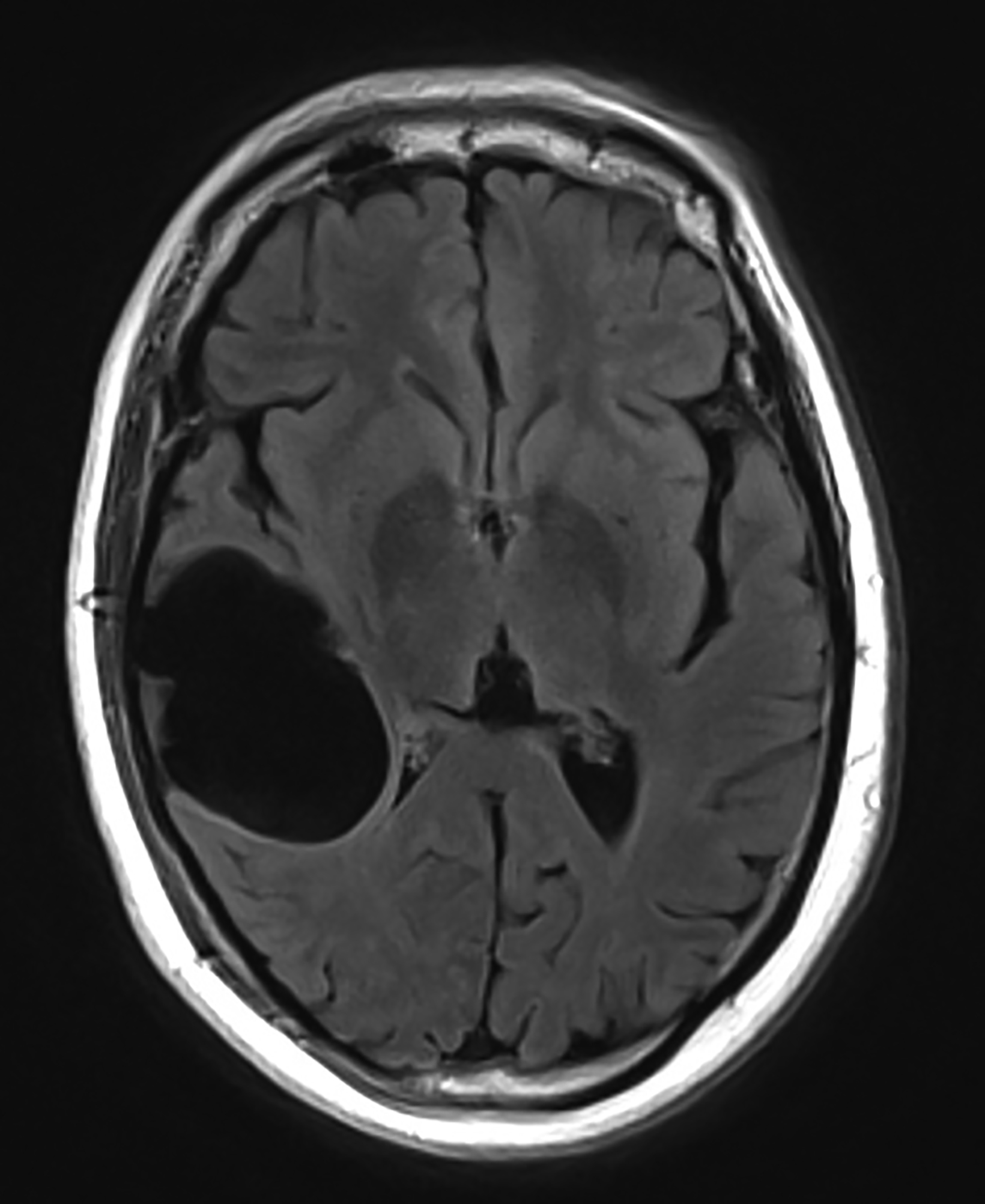
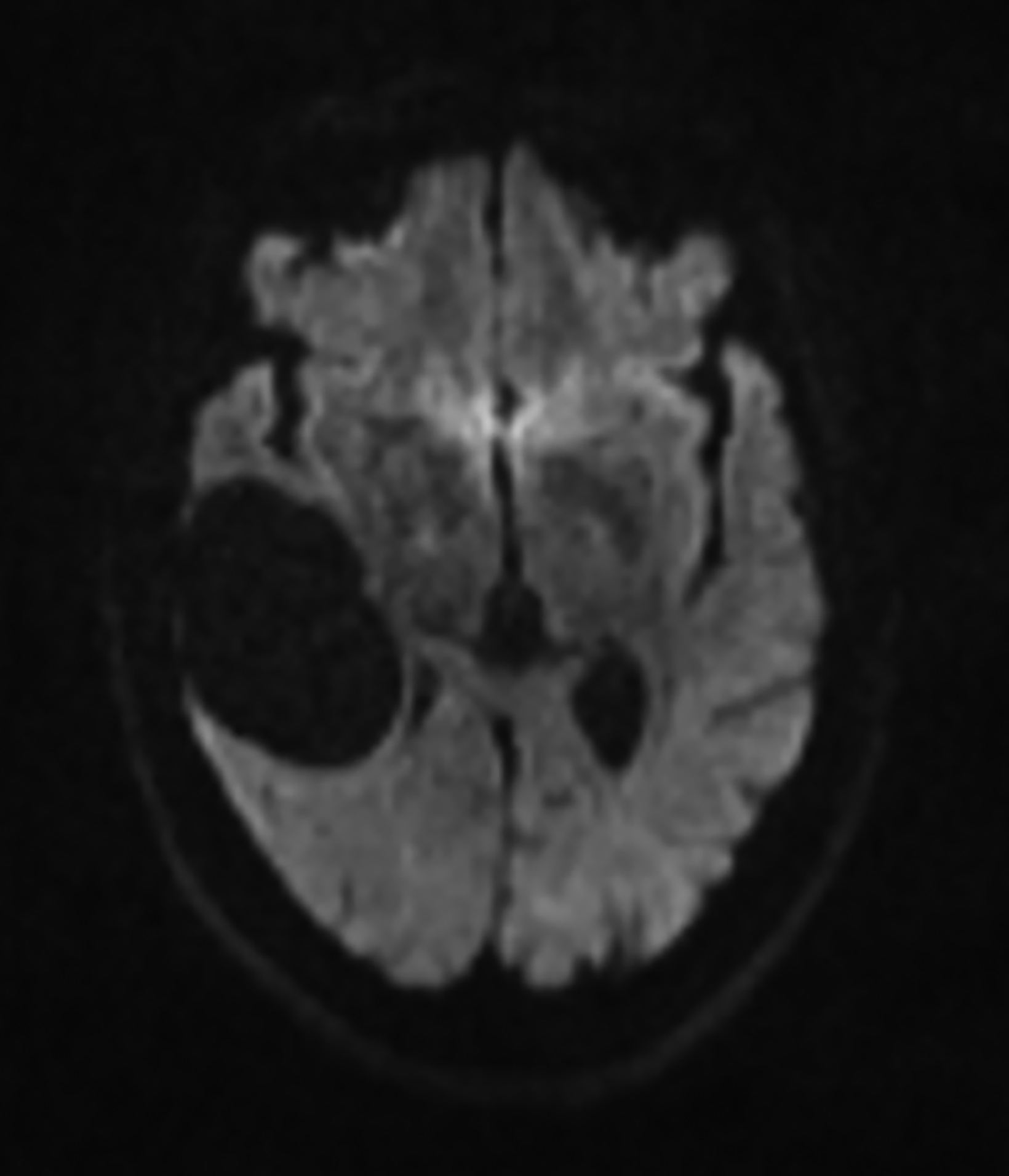
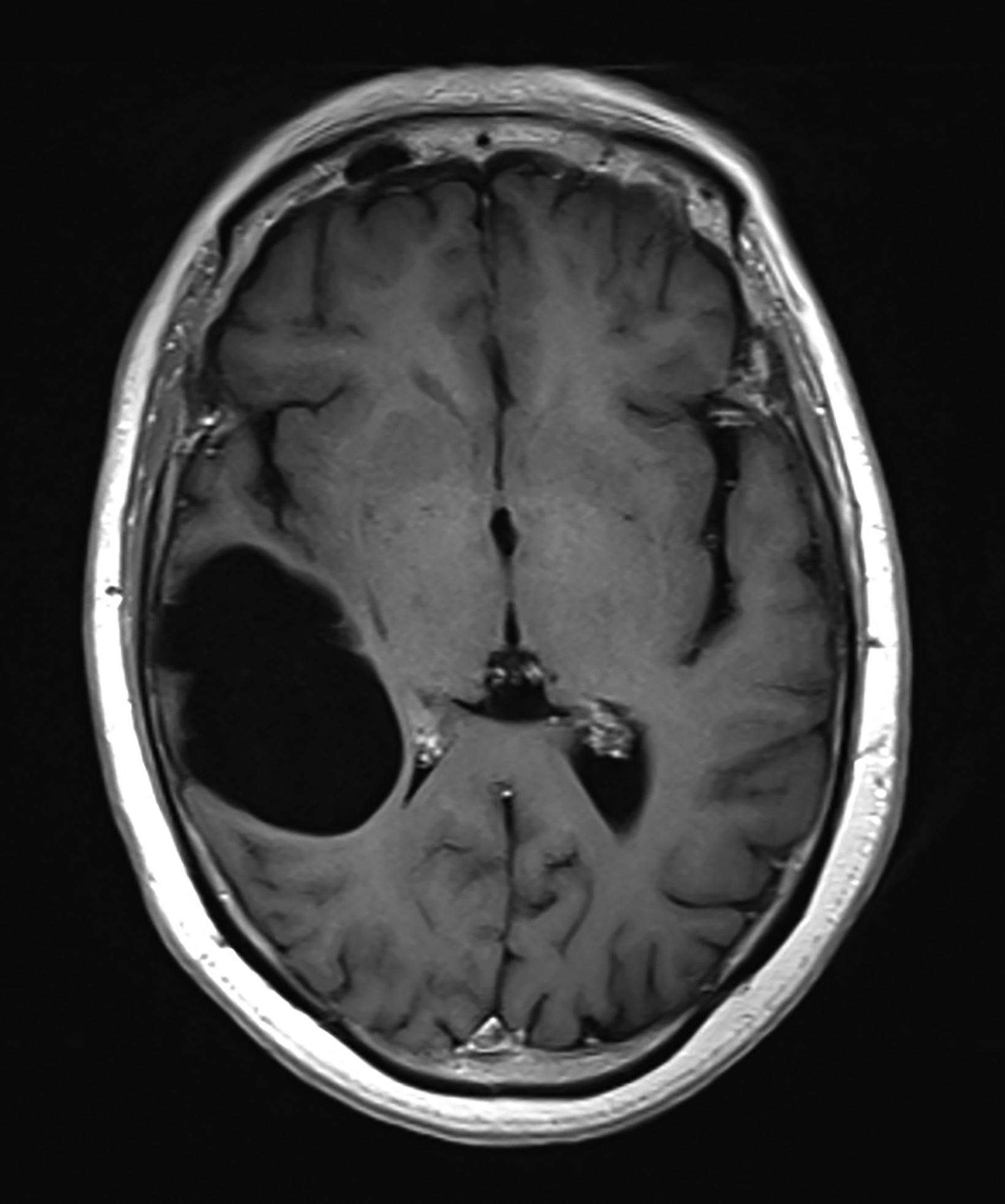
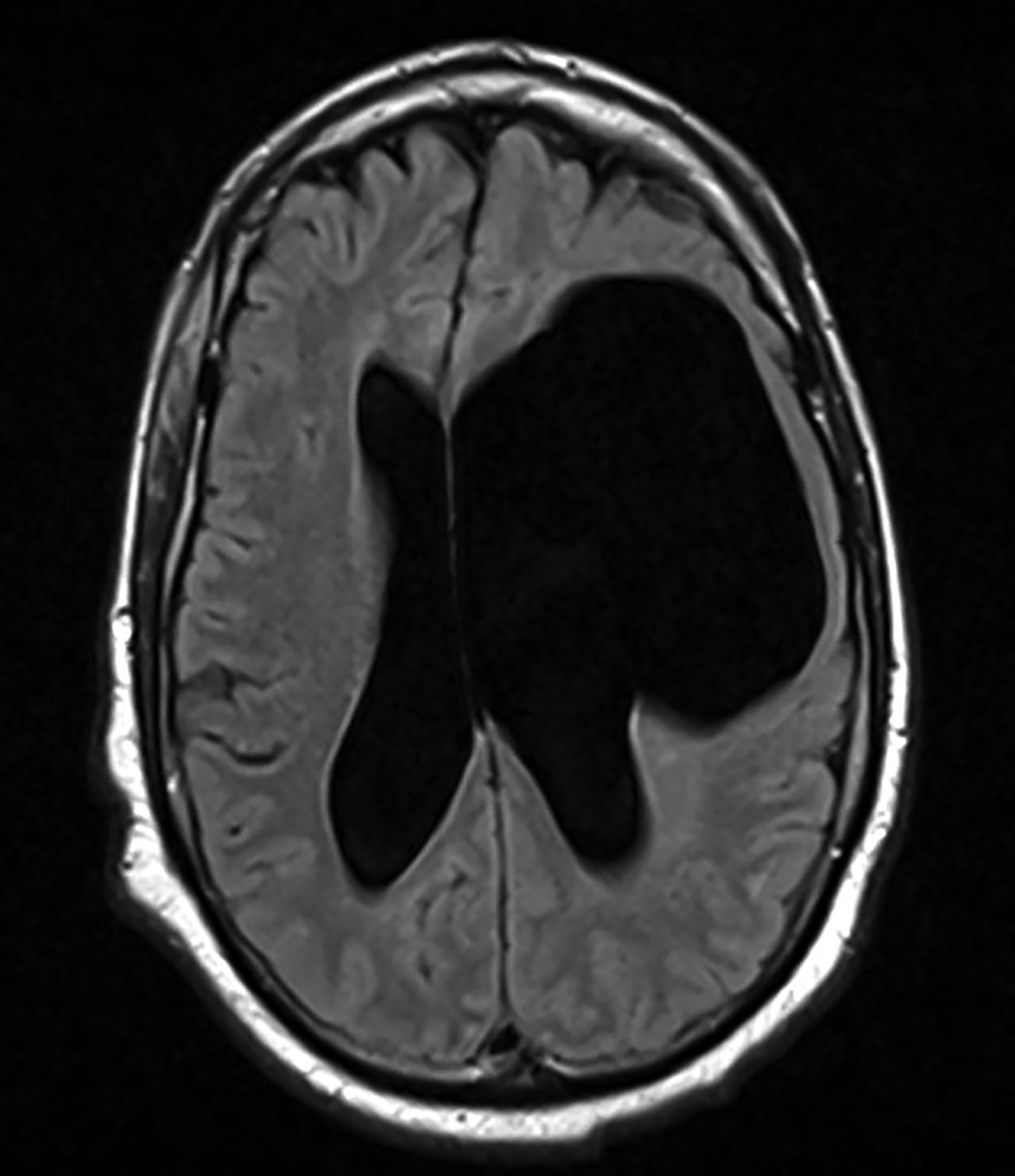
Porencephalic cysts are CSF-filled cavities that are usually contiguous with the enlarged adjacent ventricular system. However, a porencephalic cyst may be separable from the adjacent ventricle. The estimated incidence of porencephalic cysts is 3.5 per 100,000 live births.15 Porencephalic cysts develop as cystic degeneration resulting from focal encephalomalacia secondary to an insult such as ischemia, infection, trauma, surgery, and chemoradiation treatment.16,17 Mutations in the COL4A1 gene have also been reported in patients with developmental porencephaly. This gene encodes type IV collagen, a structural element of the vascular basement membrane.18
Clinical presentation varies with cyst size and location.19 Signs include seizures, language impairment, psychosis, motor deficit, developmental delay, diplopia, spontaneous CSF rhinorrhea, and otorrhea.20
Porencephalic cysts may develop a one-way valve effect whereby CSF pulsations result in slowly progressive enlargement of the cyst and subsequent remodeling of the overlying calvarium. The cysts are most commonly located in the deep cerebral white matter, but they also may be cortical or subcortical and unilateral or bilateral.21
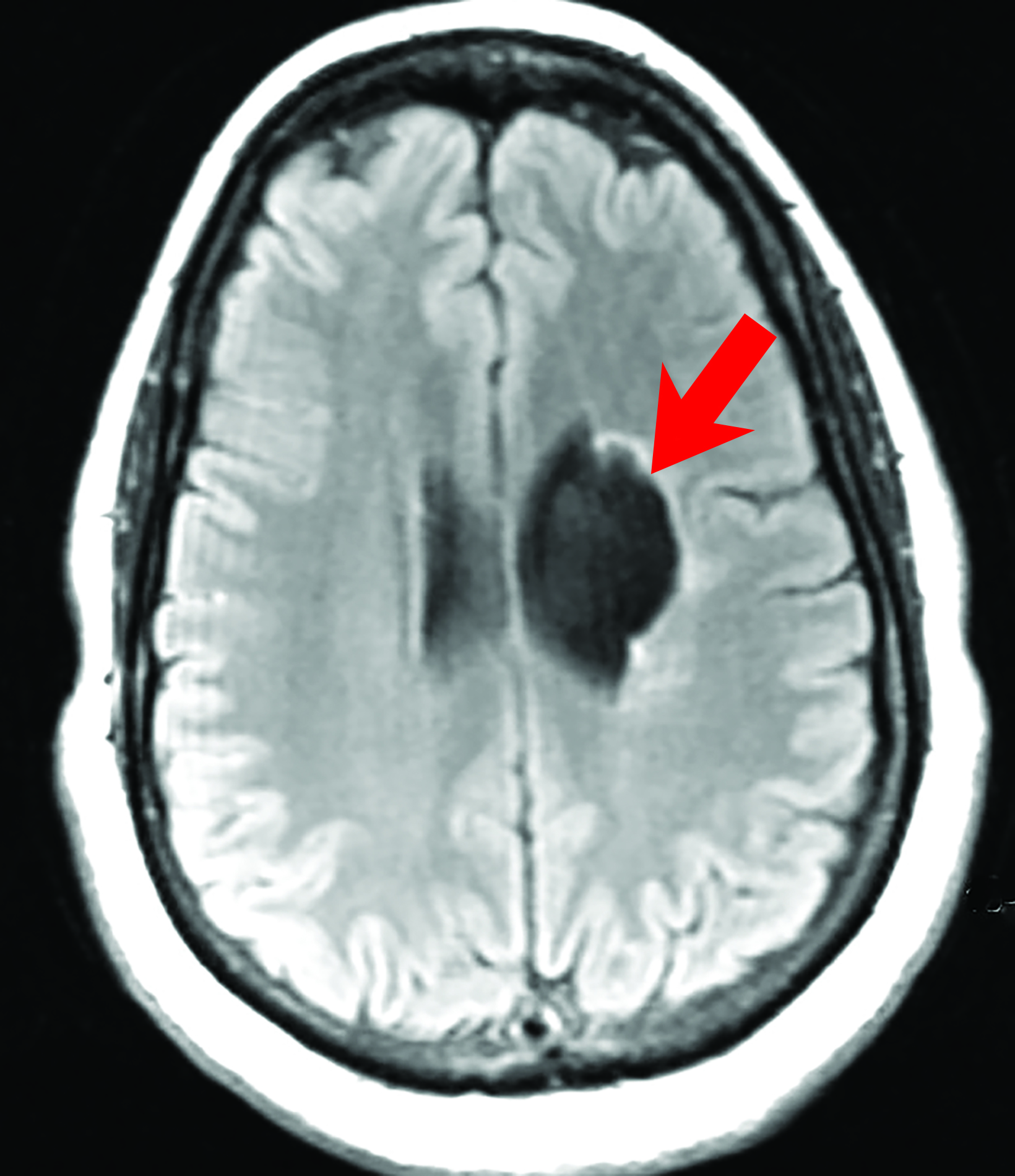
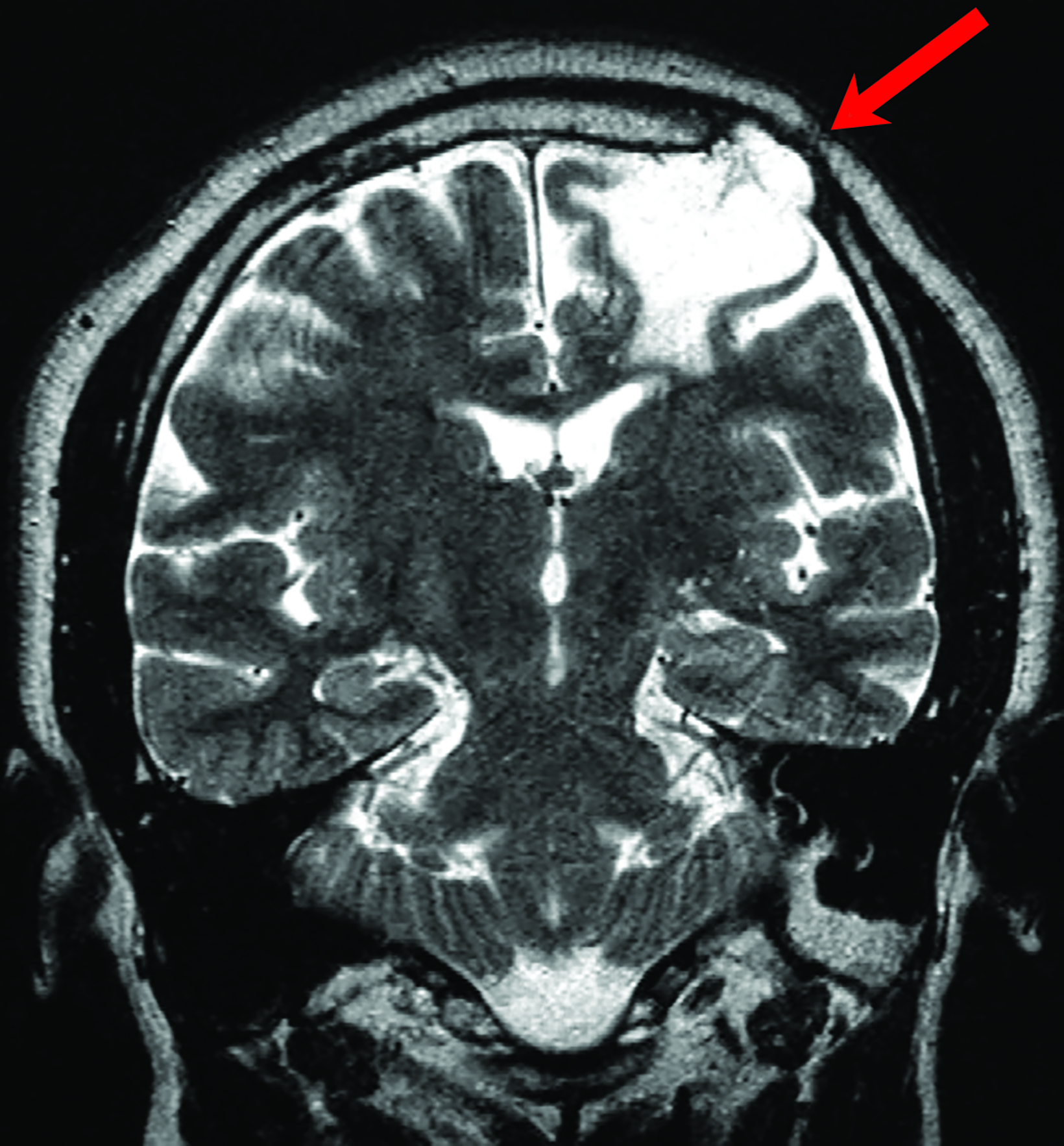
On imaging, porencephalic cysts are isodense to CSF on CT, and isointense to CSF on all MR sequences (Figure 5). There is no associated contrast enhancement or diffusion restriction. The presence of surrounding gliosis (Figure 6) differentiates porencephalic from glioependymal cysts.21
Post-traumatic Cyst
Intracerebral cysts may occur subsequent to head injury. There are two varieties of post-traumatic brain cysts: Intra-axial cysts and intradiploic, leptomeningeal cysts. The former develop soon after head injury and typically present with headache and focal deficits. They are solitary cysts with well-defined walls that may demonstrate fluid-fluid levels and/or old blood products.22
Intradiploic, leptomeningeal cysts are rare and tend to occur as a late complication of head injury in pediatric patients (Figure 7). They are usually associated with calvarial fractures.22 Intradiploic arachnoid cysts should be considered in the differential diagnosis, as they have been reported to occur after trauma and may be difficult to differentiate from post-traumatic, intradiploic, leptomeningeal cysts.22,23
Conclusion
Seen across a broad spectrum of pathology, intracranial cysts can demonstrate overlapping anatomic and imaging characteristics. However, proper knowledge of their clinical presentation, anatomic location, and imaging appearances can help to narrow the differential diagnosis and facilitate patient care.
References
- Engel U, Gottschalk S, Niehaus L, et al. Cystic lesions of the pineal region—MRI and pathology. Neuroradiology. 2000;42(6):399-402.
- Barboriak DP, Lee L, Provenzale JM. Serial MR imaging of pineal cysts: implications for natural history and follow-up. AJR Am J Roentgenol. 2001;176(3):737-743.
- Smith AB, Rushing EJ, Smirniotopoulos JG. From the archives of the AFIP: lesions of the pineal region: radiologic-pathologic correlation. Radiographics. 2010;30(7):2001-2020.
- Morigaki R, Shinno K, Pooh KH, Nakagawa Y. Giant glioependymal cyst in an infant. J Neurosurg Pediatr. 2011;7(2):175-178.
- Obaldo RE, Shao L, Lowe LH. Congenital glioependymal cyst presenting with severe proptosis. AJNR Am J Neuroradiol. 2007:999-1000.
- Robles LA, Paez JM, Ayala D, Boleaga-Duran B. Intracranial glioependymal (neuroglial) cysts: a systematic review. Acta Neurochir (Wien). 2018;160(7):1439-1449.
- Bejar JM, Kepes J, Koller WC. Hemiballism and tremor due to ependymal cyst. Mov Disord. 1992;7(4):370-372.
- Friede RL, Yasargil MG. Supratentorial intracerebral epithelial (ependymal) cysts: review, case reports, and fine structure. J Neurol Neurosurg Psychiatry. 1977;40(2):127-137.
- Naidich TP, Daniels DL, Haughton VM, Williams A, Pojunas K, Palacios E. Hippocampal formation and related structures of the limbic lobe: anatomic-MR correlation. Part I. Surface features and coronal sections. Radiology. 1987;162(3):747-754.
- Sherman JL, Camponovo E, Citrin CM. MR imaging of CSF-like choroidal fissure and parenchymal cysts of the brain. AJR Am J Roentgenol. 1990;155(5):1069-1075.
- Kjos BO, Brant-Zawadzki M, Kucharczyk W, Kelly WM, Norman D, Newton TH. Cystic intracranial lesions: magnetic resonance imaging. Radiology. 1985;155(2):363-369.
- Go KG, Hew JM, Kamman RL, Molenaar WM, Pruim J, Blaauw EH. Cystic lesions of the brain. A classification based on pathogenesis, with consideration of histological and radiological features. Eur J Radiol. 1993;17(2):69-84.
- Karatas A, Gelal F, Gurkan G, Feran H. Growing Hemorrhagic Choroidal Fissure Cyst. J Korean Neurosurg Soc. 2016;59(2):168-71.
- Naeini RM, Yoo JH, Hunter JV. Spectrum of choroid plexus lesions in children. AJR Am J Roentgenol. 2009;192(1):32-40.
- Wynne D, Abdul Jalil MF, Dhillon R. Endoscopic fenestration of a symptomatic porencephalic cyst in an adult. World Neurosurg. 2020;141:245-246.
- Ozeki M, Funato M, Teramoto T, et al. Reversible cerebrospinal fluid edema and porencephalic cyst, a rare complication of ventricular catheter. J Clin. 2010;17(5):658-661.
- Dominguez JF, Shah S, Li B, Feldstein E, Kim MG, Tobias ME. Porencephalic cyst after endoscopic third ventriculostomy and Ommaya reservoir placement: case report and review of the literature. Childs Nerv Syst. 2021; 37(9):2917-2921.
- Yoneda Y, Haginoya K, Arai H, et al. De novo and inherited mutations in COL4A2, encoding the type IV collagen α2 chain cause porencephaly. Am J Hum Genet. 2012;90(1):86-90.
- Qureshi A, Jehangir A, York EP. Porencephalic cyst: a rare cause of new-onset seizure in an adult. J Community Hosp Intern Med Perspect. 2018;8(2):92-93.
- Ryzenman JM, Rothholtz VS, Wiet RJ. Porencephalic cyst: a review of the literature and management of a rare cause of cerebrospinal fluid otorrhea. Otol Neurotol. 2007;28(3):381-6.
- Osborn AG, Preece MT. Intracranial cysts: radiologic-pathologic correlation and imaging approach. Radiology. 2006;239(3):650-64.
- Bava J, Bansal A, Patil SB, Kale KA, Joshi AR. Posttraumatic Intradiploic Leptomeningeal Cyst: A Rare Complication of Head Trauma. Case Rep Radiol. 2015;2015:395380
- Kadri H, Mawla AA. Late appearance of hydrocephalus associated with posttraumatic intradiploic arachnoid cyst. Childs Nerv Syst. 2004;20(7):494-495.
References
Citation
O K, H K, SS K, I Z. Non-neoplastic Cystic Lesions of the Central Nervous System, Part 2: Idiopathic and Acquired Cysts. Appl Radiol. 2022;(5):7-13.
August 30, 2022