MR-Guided Transurethral Ultrasound Ablation for Prostate Cancer Shows Success
Images
According to new research to be presented at the Society of Interventional Radiology Annual Scientific Meeting, minimally invasive treatment using MRI and transurethral ultrasound instead of surgery or radiation is effective in treating prostate cancer.
The traditional treatment options of radiation or surgery often come with a risk of side effects, including urinary incontinence and erectile dysfunction that cause significant morbidity and adverse lifestyle effects. Researchers said that some patients now have a durable alternative for whole-gland treatment with MRI-guided transurethral ultrasound ablation (TULSA) that does not preclude future treatment with surgery or radiation.
“The success of TULSA represents a revolution in whole-gland treatment for prostate cancer,” said lead author Steven S. Raman, MD, FASR, FSIR, professor of radiology, urology and surgery at the David Geffen School of Medicine at UCLA. “Prostate cancer is the most common form of cancer in men, affecting one in eight men in their lifetimes. We have more research to do, but if validated, TULSA has the potential to change the standard of care for thousands of men.”
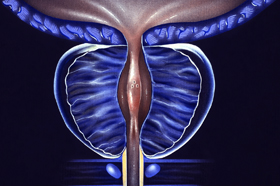
In the TULSA procedure, a small catheter-like device is inserted through the urethra into the prostate. Once there, MRI is used to guide precise positioning of 10 therapeutic ultrasound elements into the prostate. MR thermometry is used to monitor the tissue while heating to more than 55 degrees within the prostate and limiting heat to the sensitive nerves surrounding the prostate as the device rotates around the entire gland. The procedure can be performed in an outpatient or in-patient facility under general or spinal anesthesia in two to three hours.
According to Dr Raman, “This image-guided therapy maximizes our ability to kill cancer cells while minimizing collateral damage to the prostate to achieve the ultimate trifecta in prostate cancer treatment: full local cancer control while maintaining urinary continence and potency. The latter are the complications of most prostate cancer therapies that patients hate and often result from a lack of precision in treatment monitoring.”
In the prospective observational study, participants showed improvement in the reduction of the presence of cancer, prostate size and prostate-specific antigen levels (PSA), which are markers for cancer. Cancer was undetectable on follow up biopsy by 76% at one year after TULSA with a decrease in median prostate volume by 92% within one year and a decrease in PSA from 6.3 ng/ml to 0.63 ng/ml at five years.
TULSA had a very favorable side-effect profile compared to alternative surgical, radiation and thermal therapy (US guided HIFU or cryotherapy) showing that by 5 years, 92% of patients recovered continence and 87% preserved erectile function. During the study, 115 men were enrolled across 13 sites in 5 countries. Of those treated, 25 men received follow up conventional treatment with surgery or radiation because of residual or new tumors. Through this process, researchers learned the early predictors of TULSA failure related to calcifications between the urethra and target PCa and better monitoring of prostate swelling, targeting and misalignment, leading to improved detection and management of these preventable errors during the procedure.
Dr Raman noted that the study affirms that interventional radiologists (IRs) now have a meaningful role in detection and management of prostate cancer care as they already had in other types of cancer, such as lung, kidney and liver cancers. He said IRs’ expertise in imaging and image-guided procedures and experience with ablation make them a critical part of the prostate cancer care team.
The research into TULSA’s effectiveness continues with the CAPTAIN trial, a randomized control trial comparing TULSA with radical prostatectomy.