Lipofibromatous Hamartoma of the Median Nerve
Images


Case summary
An adult presented with 2-3 years of gradually increasing swelling over the distal volar aspect of the right forearm and paresthesia of the right hand (Figure 1). The patient denied any history of trauma. On physical examination, there was a palpable mass at the site of the swelling. Macrodactyly was noted involving index, middle, and ring fingers (Figure 2).
Imaging Findings
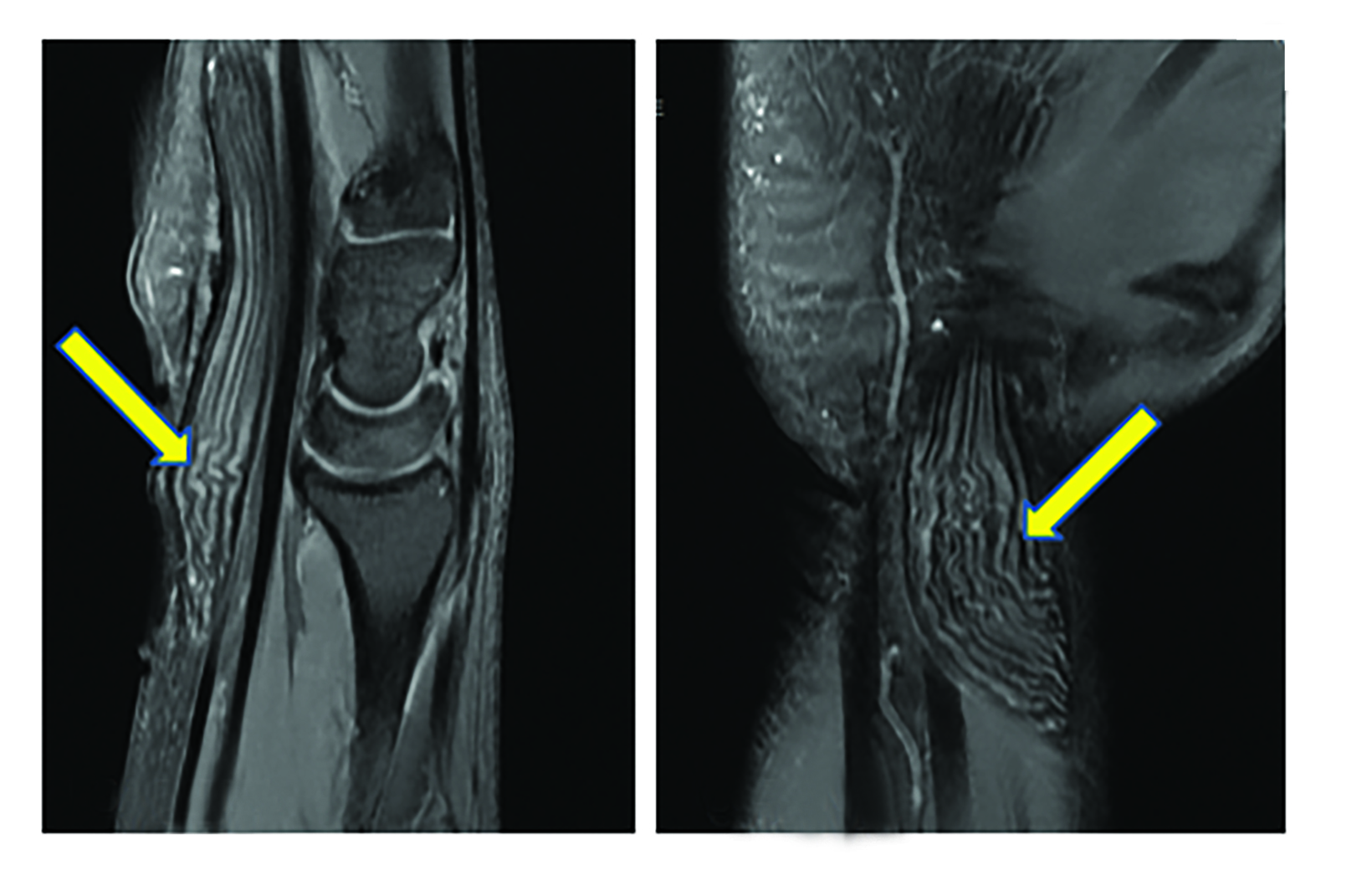
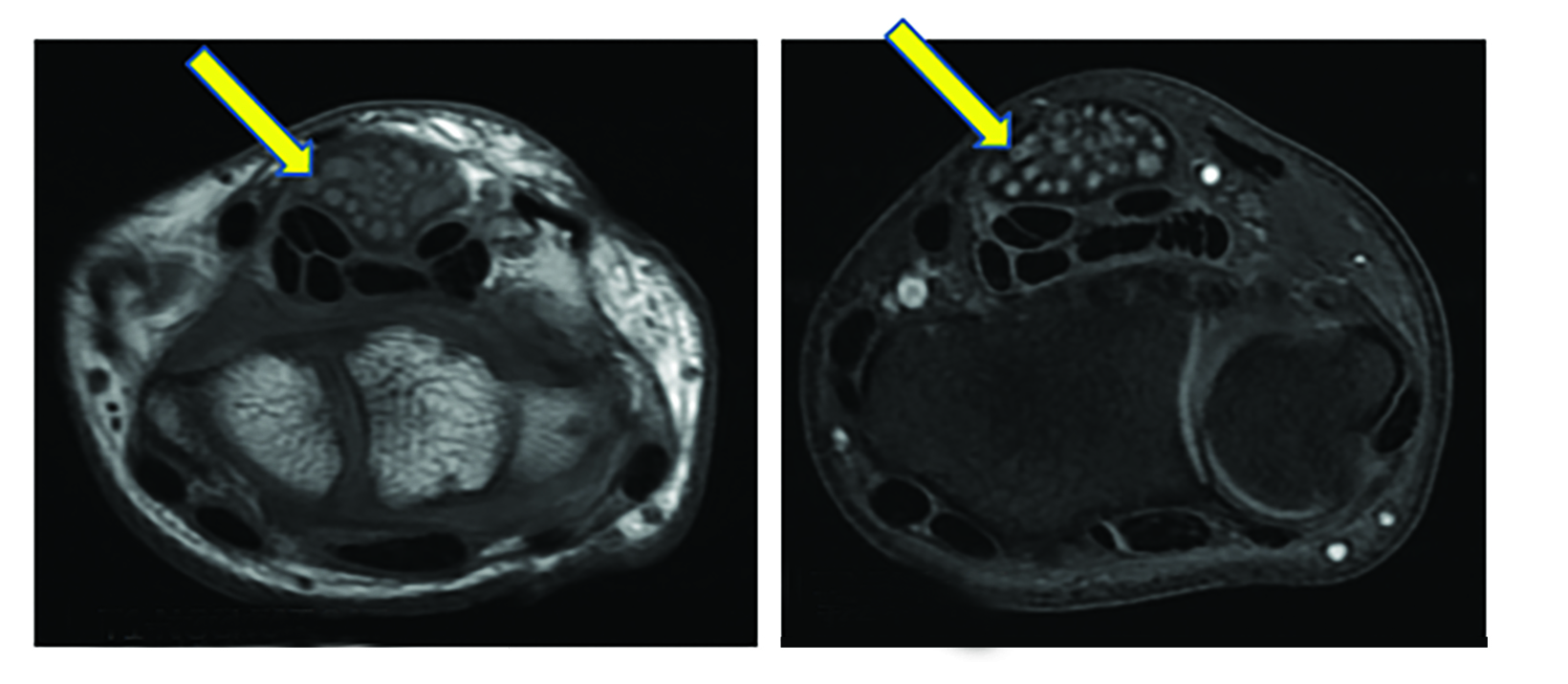
Magnetic resonance imaging (MRI) showed long segment thickening (maximum thickness 1.6 cm) of the right median nerve extending for a length of approximately 15 cm. The proximal end of this thickened segment was seen approximately 5.3 cm above the radial styloid process and the distal end at the mid aspect of the third metacarpal (Figure 3). Multiple T1 hyperintense nerve fascicles were identified giving a “coaxial cable-like” or “spaghetti string-like” appearance on T1 andT2 images (Figure 4). There was mild suppression of T1 hyperintense areas on fat-suppressed images (Figure 4), suggesting the presence of fat. No post-contrast enhancement was noted on subtracted images.
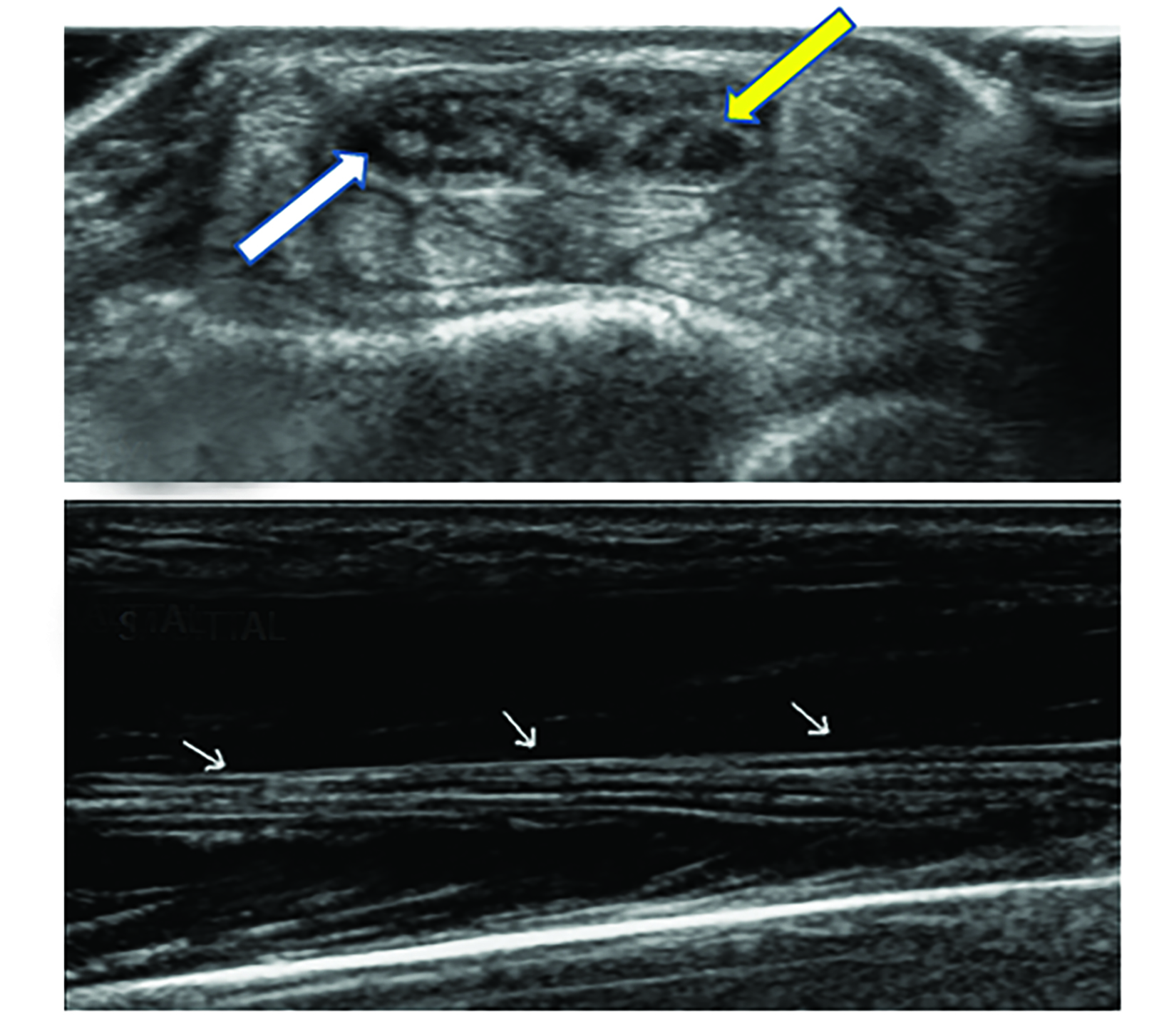
Ultrasound showed thickening of the median nerve with nerve fascicles surrounded by hyperechoic fibrofatty tissue (Figure 5).
Diagnosis
Lipofibromatous hamartoma of the median nerve
Discussion
Neurogenic lipofibromatous hamartoma is a rare, slow-growing, benign tumor. It is designated as nervous lipomatosis as per the new World Health Organization classification of tumors.1 Other nomenclature includes neural fibrolipoma, perineural lipoma, and intraneural lipoma.2 This condition is best described by the term intraneural lipoma, first used in 1964 by Morley.3 Its incidence has not been mentioned in the literature.4 There is a predominance of cases in infants with adult cases described up to the age of 40.3 There is a male gender predilection.
The pathophysiology of this entity is distortion and enlargement of the epineurium and perineurium, owing to excessive fatty and fibrous tissue that infiltrates between as well as around the nerve fascicles; however, the individual nerve fibers are usually normal.3
The median nerve is the most commonly involved nerve, and it often presents as carpal tunnel syndrome.5 The radial, ulnar, dorsal foot, and brachial plexus nerves can also be involved.1
Patients generally present with swelling at the site and sensory and motor deficits due to compression of the neural component.1 Approximately two-thirds of cases also have macrodactyly, which has a female predilection.3,4
>Magnetic resonance imaging and ultrasonography are the preferred imaging modalities for evaluation. On ultrasonography, intraneural soft tissue appears hyperechoic as compared to compressed and relatively hypoechoic nerve fibrils.1,5 Pathognomonic on MRI, features include enlargement of the affected nerve with multiple T1 hypointense nerve fascicles, giving a “coaxial cable-like” or “spaghetti string-like” owing to surrounding T1 and T2 hyperintense fatty tissue.4,6 This distinctive appearance on MRI usually leads to a specific diagnosis and eliminates the need for tissue sampling.2,5
Treatment includes tenotomy and fasciotomy but depends on a confident diagnosis; differential diagnoses such as lipoma or neurofibroma must be carefully ruled out. A conservative approach is preferred whenever possible.6
Conclusion
Lipofibromatous hamartoma of the median nerve is a rare benign tumor that causes distortion of the epineurium and perineurium due to excessive fatty and fibrous tissue that infiltrates between and around the nerve fascicles, Individual nerve fibers, however, are usually normal. A “coaxial cable-like” or “spaghetti string-like” appearance on MRI is typical of this entity and can obviate the need for tissue diagnosis.
References
- Bansal A, Verma A, Mourya C. Fibrolipomatous hamartoma of median nerve: A rare cause of carpal tunnel syndrome and macrodactyly. J Orthop Allied Sci 2015;3:63-64.
- Gilet A, Jeremy M, Gould E. Fibrolipomatous Hamartoma of the Median Nerve. Radiol Case Rep. 2015;3(3):195. Published 2015 Nov 6. doi:10.2484/rcr.v3i3.195
- Louaste J, Zejjari H, Chkoura M, Houmadi A, Rachid K. Carpal tunnel syndrome due to fibrolipomatous hamartoma of the median nerve. Hand (N Y). 2011;6(1):76-79.
- Shekhani HN, Hanna T, Johnson JO. Lipofibromatous Hamartoma of the Median Nerve: A Case Report. J Radiol Case Rep. 2016;10(11):1-7. Published 2016 Nov 30. doi:10.3941/jrcr.v10i11.2787
- Toms AP, Anastakis D, Bleakney RR, Marshall TJ. Lipofibromatous hamartoma of the upper extremity: a review of the radiologic findings for 15 patients. AJR Am J Roentgenol. 2006;186(3):805-811.
- Senger JL, Classen D, Bruce G, Kanthan R. Fibrolipomatous hamartoma of the median nerve: A cause of acute bilateral carpal tunnel syndrome in a three- year-old child: A case report and comprehensive literature review. Plast Surg (Oakv). 2014;22(3):201-206.
References
Citation
PC T, M V, D P, G R,. Lipofibromatous Hamartoma of the Median Nerve. Appl Radiol. 2022;(5):41-43.
August 31, 2022