Limy Bile Syndrome
Images
Case Summary
An adult with cirrhosis due to hepatitis C infection was referred for abdominal imaging.
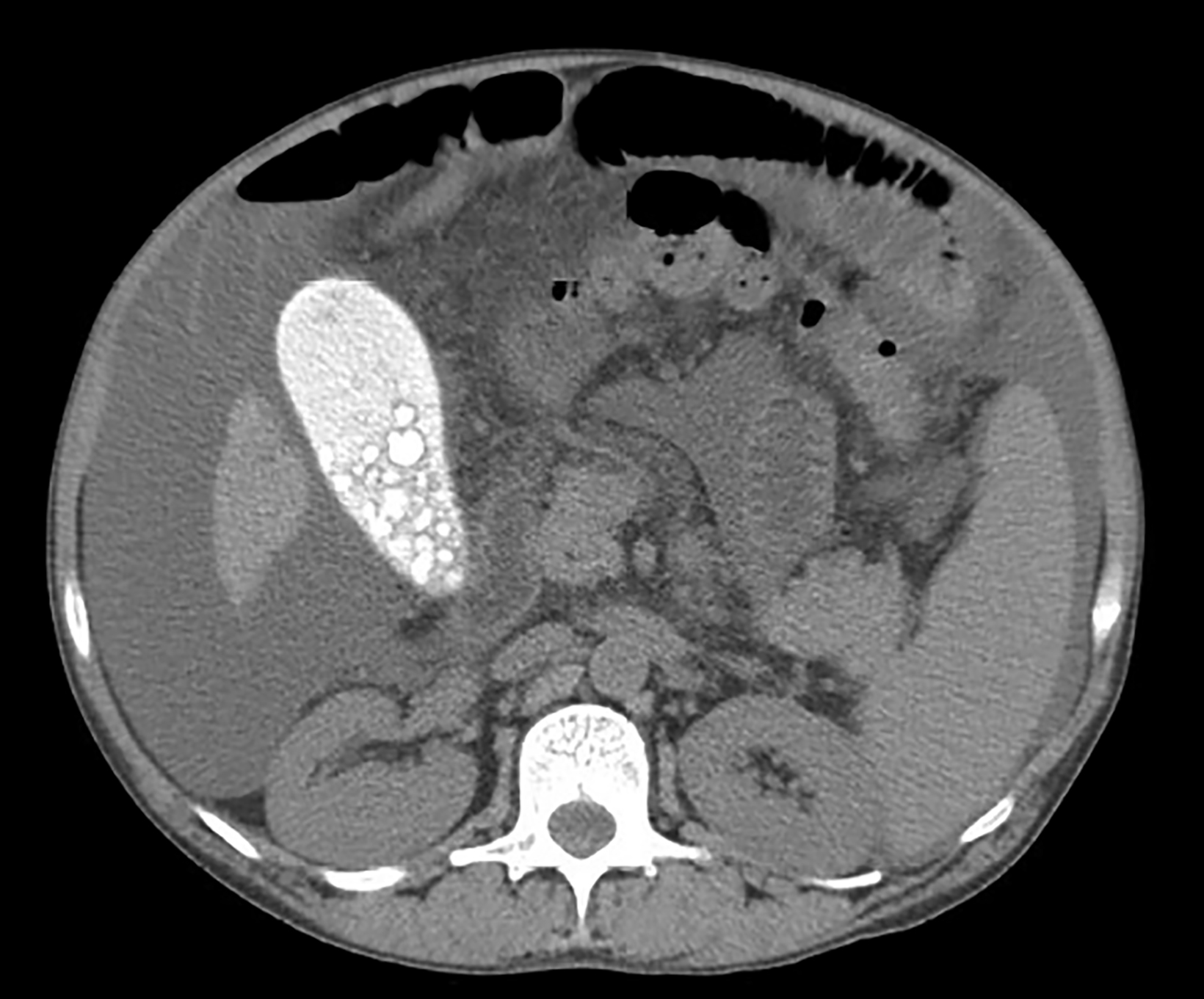
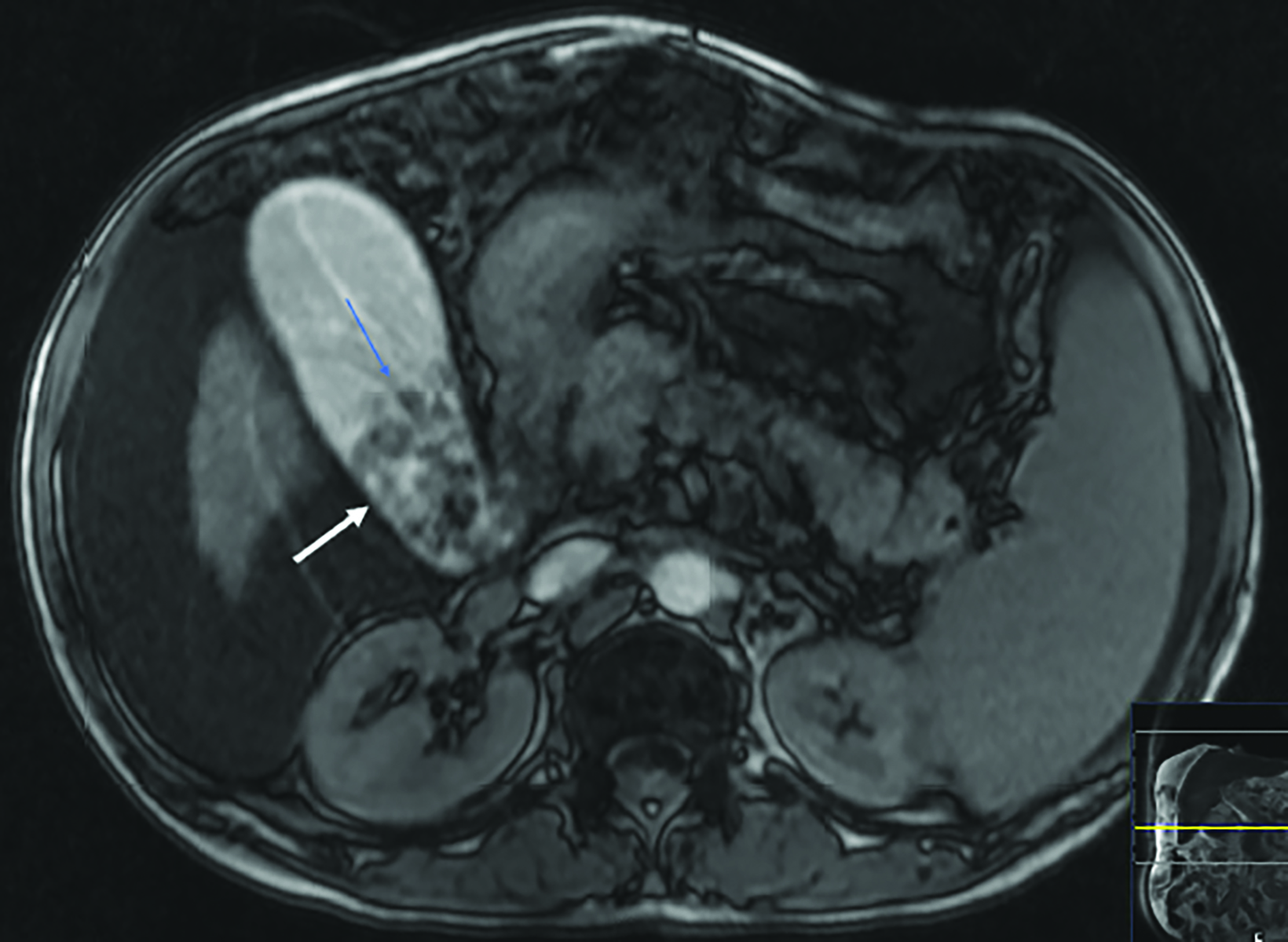
Computed tomography (CT) revealed a large, radiopaque gallbladder containing numerous calculi. A nodular liver and ascites were also present. Magnetic resonance imaging (MRI) showed cholelithiasis and an enhancing lesion of the right hepatic lobe consistent with hepatocellular carcinoma.
Imaging Findings
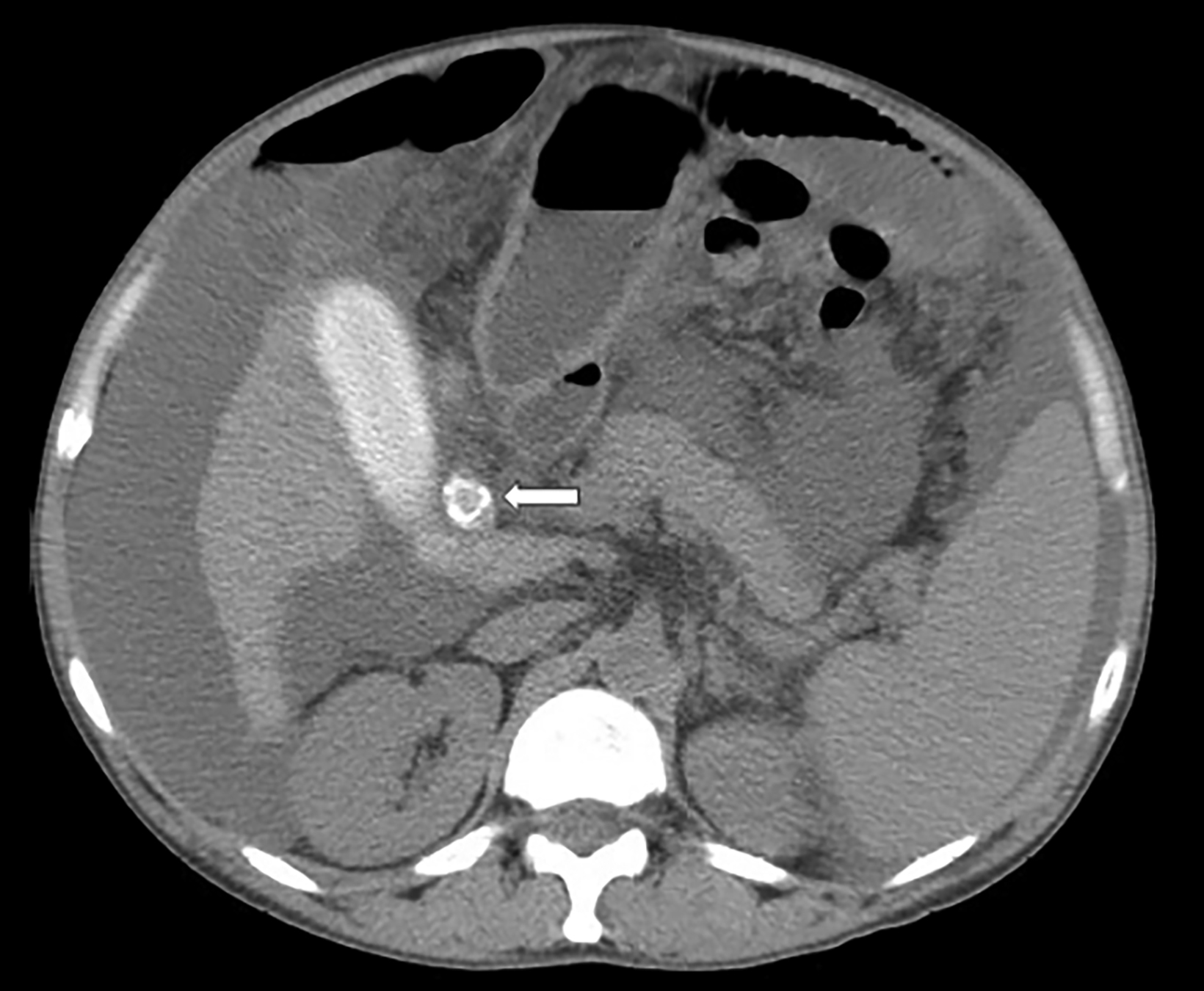
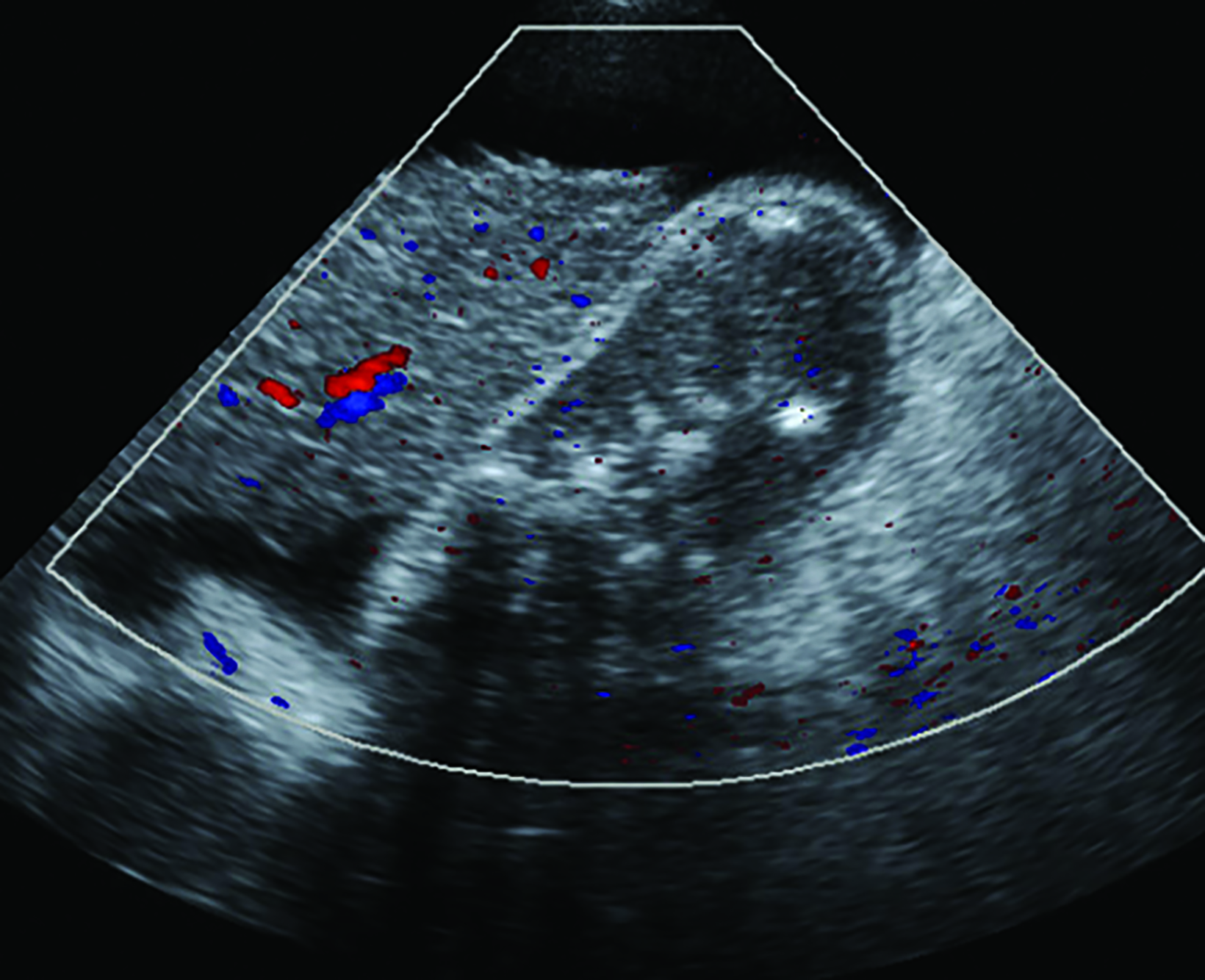
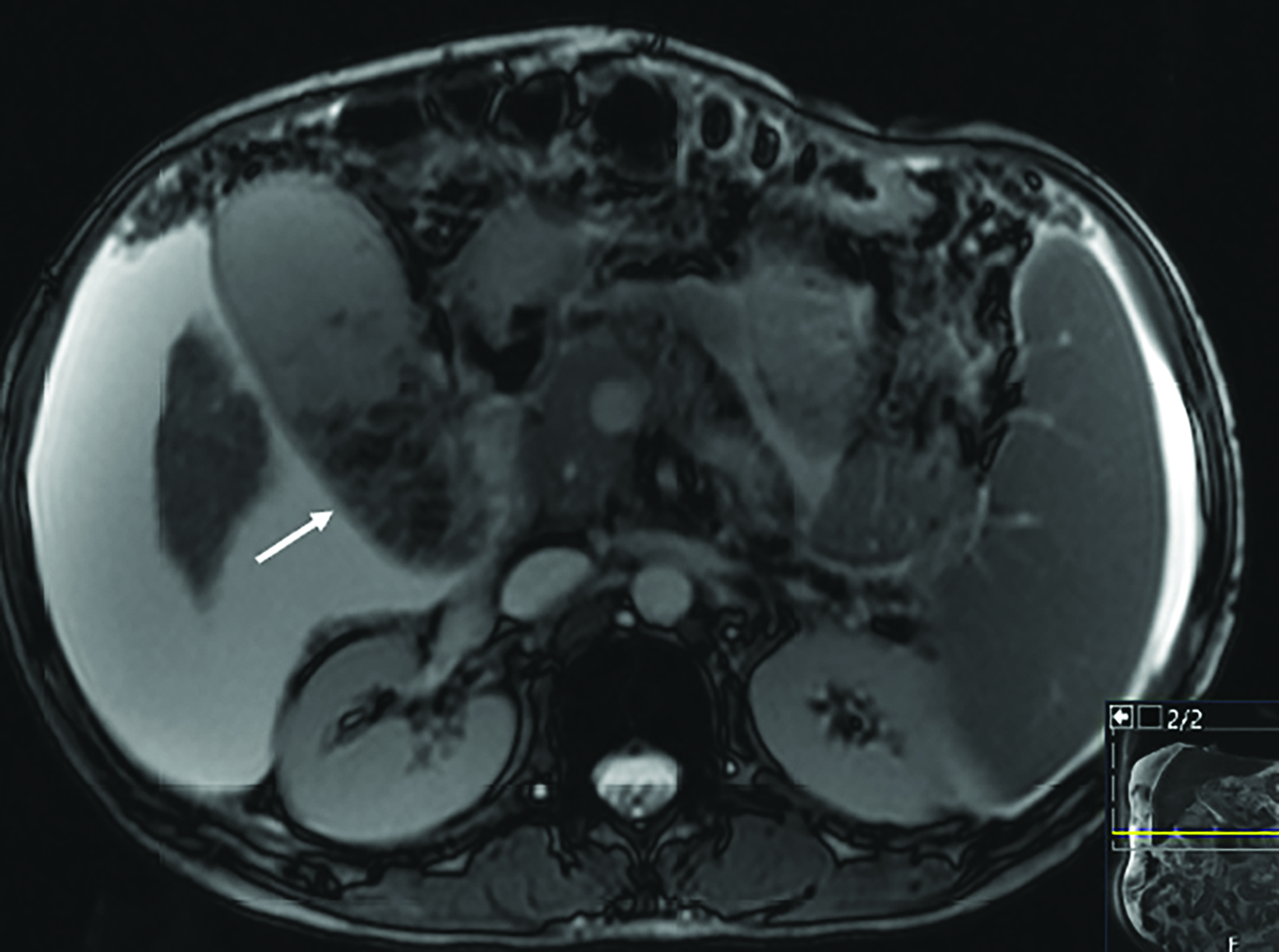
Precontrast CT showed a distended gallbladder measuring 10.2 cm in length and 4 cm in diameter, filled with markedly radiopaque content (184 HU). The gallbladder contained many small calculi and its neck was blocked by a 1.2 cm impacted stone. A cirrhotic liver and massive ascites were also visible (Figure 1). Ultrasonography of the gallbladder redemonstrated the cholelithiasis, but there was no pain or tenderness on palpation (Murphy sign) to indicate cholecystitis (Figure 2). MRI obtained 4 months later showed the abnormal gallbladder and ascites, as well as a 1.6 cm enhancing lesion in segment 8 of the right hepatic lobe that represented a hepatocellular carcinoma (Figure 3). This tumor was treated twice with transarterial embolization (TACE) prior to liver transplantation.
Diagnosis
Limy bile syndrome.
The differential diagnosis includes gallbladder opacification by contrast material following oral cholecystography or endoscopic retrograde cholangiography, vicarious excretion due to renal or hepatic failure, and porcelain gallbladder.
Discussion
Limy bile syndrome (LBS), also known as milk-of-calcium gallbladder, is a rare idiopathic condition usually recognized by its distinct radiological features.1-3 The condition is characterized by dense opacification of the gallbladder, and seldom the bile ducts, with a creamy solution of calcium salts in the form of carbonate, oxalate, phosphate, or bilirubinate. The underlying pathogenesis is believed to be abnormal metabolism of calcium and low pH of excreted bile.4 In most of the reported cases the gallbladder had been obstructed by an impacted stone in its neck or cystic duct. Limy bile syndrome can be associated with hyperparathyroidism, chronic cholecystitis, gallstone-induced pancreatitis and, in very rare instances, gallbladder cancer or cholangiocarcinoma.5,6
This entity is usually diagnosed in patients older than 40 years, with a 3:1 female-to-male ratio.4 Only a few cases have been reported in pediatric patients.7 Most patients with LBS are asymptomatic; the condition is detected incidentally on imaging studies performed for unrelated abdominal disorders.1,8 However, some patients present with right subcostal pain, fever, and jaundice resulting from concurrent cholecystitis or biliary obstruction by gallstones.1,6
The typical finding on abdominal radiography and CT is that of a densely radiopaque gallbladder filled with a highly viscous substance, intraluminal calculi, and often obstructed by an impacted gallstone in its neck or cystic duct. Sonography and MRI can demonstrate cholelithiasis and associated ascites or pathological processes of the liver as in this case.1-4
The recommended treatment is cholecystectomy.1,6 This operation is usually performed electively, to prevent future complications. Spontaneous resolution through discharge of abnormal gallbladder content into the duodenum has been reported in a few isolated instances.8-10
Conclusion
Abdominal radiography and cross-sectional imaging modalities play a crucial role in the diagnosis of limy bile syndrome and evaluation of its associated pathological processes. This case report highlights the unique clinical and imaging features that help in the recognition and management of this rare entity.
References
Citation
GG G. Limy Bile Syndrome. Appl Radiol. 2024;(2):42-44.
March 5, 2024