Inflammatory Pseudotumor of the Nasopharynx
Images


CASE SUMMARY
An 87-year-old former smoker presented with severe unrelenting headache following trivial trauma. The patient also had developed recent onset facial numbness and facial palsy. Medical history included hypertension and hypothyroidism, with occasional alcohol ingestion. On examination, patient was cachectic with evidence of muscle wasting but examination was otherwise normal. There was no lymph node enlarge ment. Nasal examination was suspicious for a left nasopharyngeal mass, which was confirmed by nasopharyngeal endoscopy. Two biopsies of the nasopharyngeal mass demonstrated only fibrous tissue and mild chronic inflammation with no evidence of malignancy.
IMAGING FINDINGS
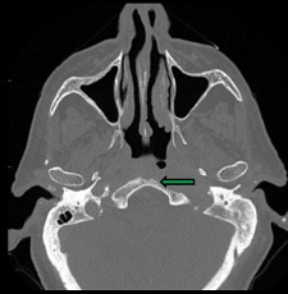
Nasopharyngeal inflammatory pseudotumor (IPT) appears as homogeneously enhancing nasopharyngeal soft tissue on contrast-enhanced CT examination. Associated destruction of the skull base (Figure 1) and narrowing of the neighboring skull base foramina/canals may occur. There is usually no enlargement of the cervical lymph nodes.
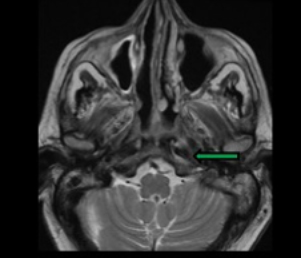
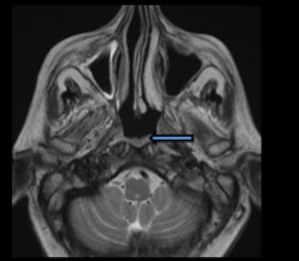
On MRI, IPTs are typically ill-defined, infiltrative masses (Figure 2) with moderate, homogeneous contrast enhancement. There is involvement of the submucosa of the nasopharynx with preservation of normal hyperintense signal of the nasopharyngeal mucosa. Contiguous structures that may be involved include the clivus, eustachian tube, carotid and parapharyngeal spaces, Meckel cave, orbital apex, and cavernous sinus. Encasement of the internal carotid artery may occur. Ipsilateral opacification of the mastoid air cells is a common finding due to eustachian tube obstruction.
DIAGNOSIS
Inflammatory pseudotumor (IPT) of the nasopharynx.
Differential diagnosis includes nasopharyngeal carcinoma (NPC), chordoma, chondrosarcoma, skull base lymphoma, plasmacytoma, and metastasis. Rosai-Dorfman disease, Epstein-Barr virus-related inflammatory pseudotumor, calcifying fibrous pseudotumor, and sclerosing lymphoma are less likely considerations.
DISCUSSION
Inflammatory pseudotumor (IPT) of the nasopharynx is a benign, idiopathic disease usually mistaken for a neoplasm/infection owing to its aggressive appearance1,2,3 Patients routinely present with recent history of otitis media, hearing loss, and/or single or multiple cranial nerve neuropathies.2
IPT is an inflammatory lesion of unknown etiology. Various theories, including autoimmune reaction linked to viral infection, infectious process due to sinusitis, or syphilis and aberrant production of fibrogenic cytokines, have been proposed.1 However, recent studies have suggested cytogenetic clonal abnormality and anaplastic lymphoma kinase expression, suspicious for a neoplastic cause.4
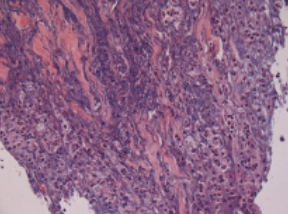
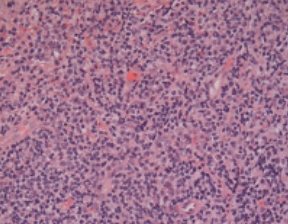
On gross pathology, IPTs resemble inflamed fibrous tissue with contiguous reactive bone. Routine microscopy demonstrates mixed acute/chronic inflammatory cells and spindle cells with a densely fibrotic background.5,6 (Figure 3).
On MRI, IPT is typically seen as a mass which is T2 hypointense compared to brain parenchyma (Figure 2), while NPC (the most common differential diagnostic consideration) is more hyperintense on T2 imaging.1,4 Internal carotid artery encasement and narrowing of the vessel lumen are common features with IPT.1 In comparison to NPC, IPT involves the submucosal layer of the nasopharynx. The hyperintense mucosal layer is well-delineated from the hypointense submucosal lesion on T2 imaging (Figure 2). Extensive pachymeningeal thickening and enhancement is a more common feature of IPT but not of NPC. Cervical lymphadenopathy is more commonly encountered in patients with NPC than with IPT.1,2,6 Systemic steroids are the treatment of choice in patients with IPT involving the nasopharynx and skull base.7
CONCLUSION
Inflammatory pseudotumor of the nasopharynx is a rare mimicker of nasopharyngeal carcinoma and other neoplastic and infectious lesions involving the skull base.
REFERENCES
- Lu CH, Yang CY, Wang CP, et.al. Imaging of nasopharyngeal inflammatory pseudotumours: differential from nasopharyngeal carcinoma. Br J Radiol. 2010 Jan;83(985):8-16,
- Chwang WB, Jain R, Narayan A, et.al. Inflammatory pseudotumor of the nasopharynx and skull base: mimicking an aggressive neoplasm or infection. Arch Otolaryngol Head Neck Surg. 2012 Aug;138(8):765-9
- Gadde J, Franck B, Liu X, et.al. Inflammatory pseudotumor of the nasopharynx with spread along the trigeminal nerve. Am J Otolaryngol. 2013 May-Jun;34(3):252-4
- Park SB,Lee JH, Weon YC. Imaging findings of head and neck inflammatory pseudotumor. AJR Am J Roentgenol. 2009 Oct;193(4):1180-6
- Han MH, Chi JG, Kim MS, et al. Fibrosing inflammatory pseudotumors involving the skull base: MR and CT manifestations with histopathologic comparison. AJNR Am J Neuroradiol. 1996 Mar;17(3):515-21
- Choi SY, Yu IK, Han MH, et.al. Fibrosing inflammatory pseudotumor of the nasopharynx: MR features and histopathologic correlation. Eur J Radiol. 2009 Nov;72(2):274-7
- Lee DK, Cho YS, Hong SH, et.al. Inflammatory pseudotumor involving the skull base: response to steroid and radiation therapy. Head Neck Surg. 2006 Jul;135(1):144-8
Citation
JKR N, R S, C D, R D C, J C,. Inflammatory Pseudotumor of the Nasopharynx. Appl Radiol. 2021;(2):48A-48B.
March 11, 2021