Imaging Upper Extremity Injuries in Pediatric Athletes
Images













SA-CME credits are available for this article here.
While many sports injuries in young athletes are similar to those in adults, several are distinct. In the skeletally immature population, the weakest areas of the skeleton are the cartilaginous physes of the epiphyses and apophyses, followed by the bones and the ligaments. As such, the cartilaginous structures are particularly prone to injury.1-4
Pediatric athletic injuries include acute traumatic fractures and chronic overuse injuries from repetitive stress. Acute injuries, such as those from direct blows or from falls on outstretched arms, are common among gymnasts, football players and wrestlers. Chronic or repetitive injuries are most common in sports that entail overhead movements, including baseball, football, tennis, and gymnastics.1,3 Radiography remains the primary imaging modality for evaluating sports-related injuries of the upper extremities. Magnetic resonance imaging (MRI), however, has a role in evaluation where there is a high clinical suspicion of injury but radiographic findings are subtle or non-diagnostic. MRI can also be used to diagnose and guide management of osteochrondral lesions.
This article focuses on the imaging of common acute and chronic sports-related upper-extremity injuries in pediatric athletes.
Acute and Chronic Injuries of the Shoulder
The shoulder is among the most common sites of acute injury in skeletally immature athletes; physeal fractures of the distal clavicle and the coracoid process are frequent.1-4 Radiographic evaluation requires at least two orthogonal views, such as true anteroposterior and axillary lateral or scapular lateral views.
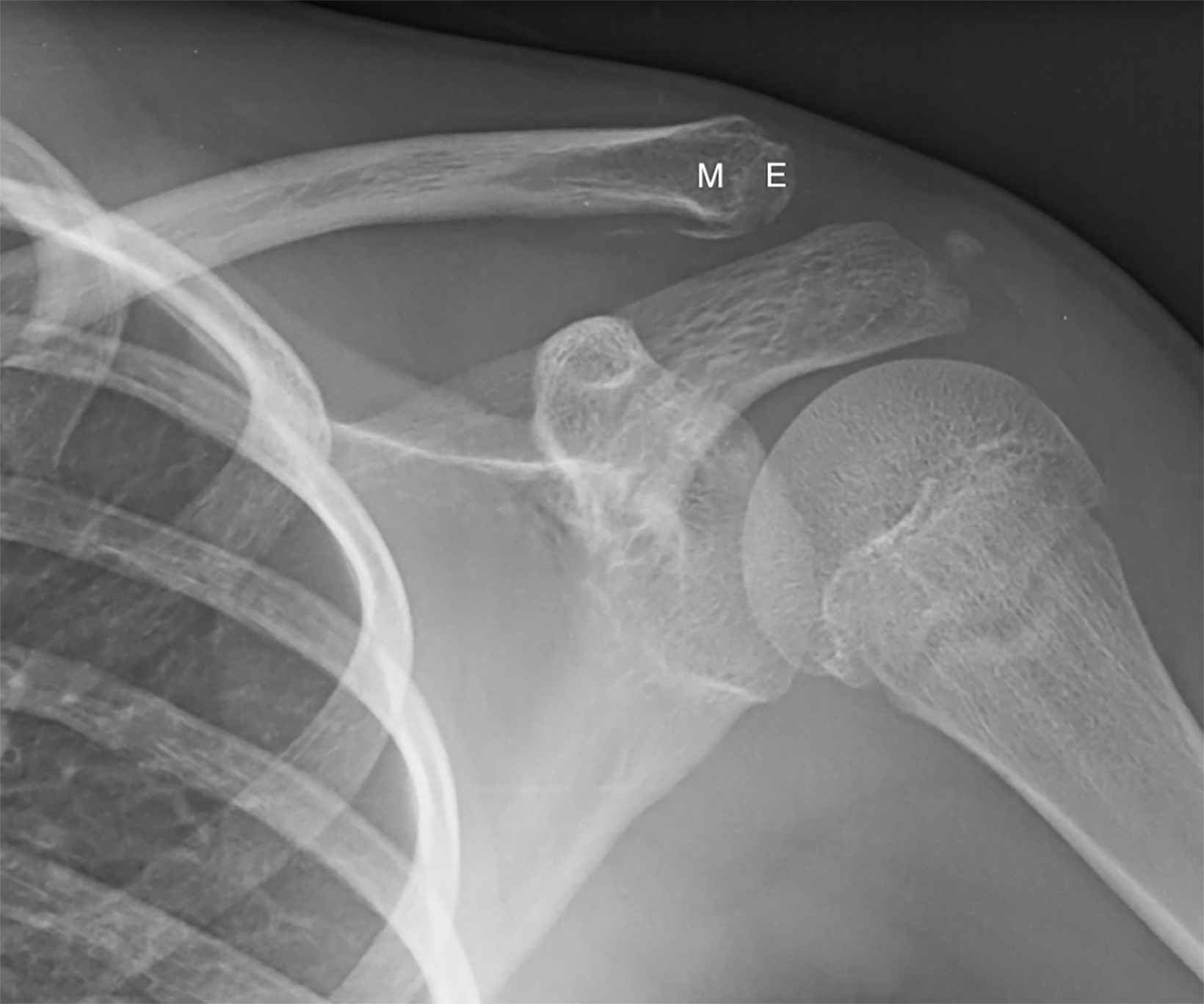
Salter-Harris I physeal fractures through the distal clavicle are caused by falling onto an outstretched arm or sustaining a direct blow to the shoulder. Radiographically, these fractures may appear very similar to an acromioclavicular separation. Recognizing these fractures is important because their prognosis is better than a true acromioclavicular separation, which may disrupt the acromioclavicular or coracoclavicular ligaments. Affected patients, typically younger than 13 years, present with acute lateral shoulder pain. Radiographic findings vary with the extent of periosteal disruption, which can range from a minimally displaced periosteal fragment to clavicular displacement in cases involving large tears in the periosteal sleeve.1,4 The distal clavicular epiphysis is non-displaced and remains in anatomic alignment with the acromion (Figure 1). These fractures usually heal with minimal if any motion limitation following shoulder immobilization.1,3
Coracoid fractures involve the physis at the base of the coracoid process. Typically occurring in football players between 13 and 15 years old, these injuries usually result from a direct blow to the shoulder.5 Radiographic findings include widening of the coracoid physis consistent with a Salter-Harris type I injury (Figure 2). Physeal fractures can be subtle; lateral scapular or Y views or MRI can enhance conspicuity of the physeal widening. Non-displaced fractures are managed conservatively, while displaced fractures may require surgery .
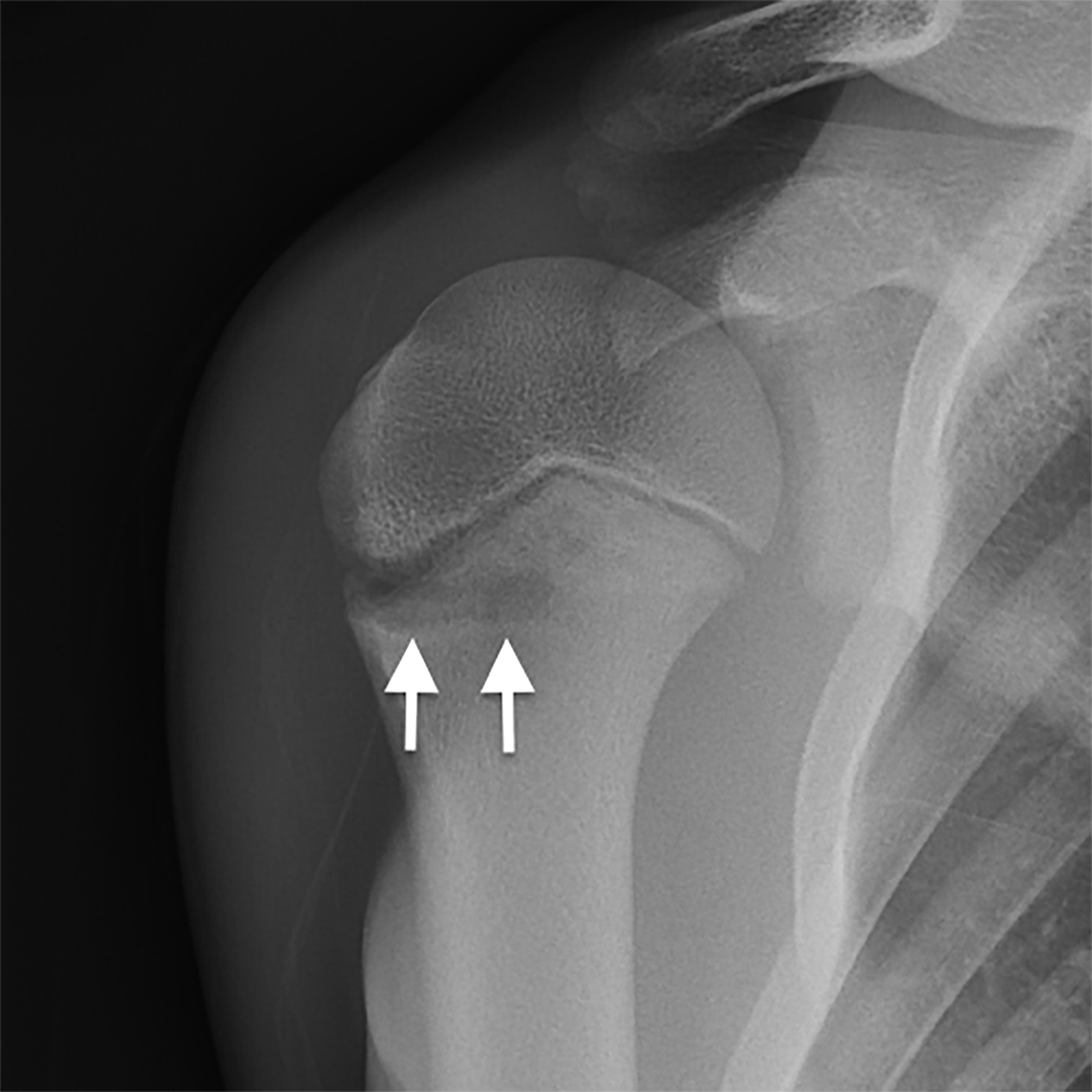
Among chronic repetitive shoulder injuries, “Little League shoulder” is the most common. The term refers to chronic valgus stress injuries in overhead throwers, most often in baseball players ages 11 to 16. Patients typically present with pain in the lateral aspect of the shoulder that worsens with throwing. Widening of the lateral aspect of the proximal humeral physis is a characteristic radiographic finding, owing to proliferation of the physeal cartilage from chronic repetitive microtrauma (Figure 3).2-4, The injury is also frequently referred to as a chronic Salter-Harris I fracture. There may be associated metaphyseal sclerosis and cystic change. The prognosis is excellent with early treatment, which consists of temporarily discontinuing throwing. Treatment delay or noncompliance may lead to osseous bridges in the physis that can alter or arrest growth.
Acute and Chronic Injuries of the Elbow
Medial epicondyle and lateral condyle fractures are among the most common acute elbow injuries in young athletes. Two views of the elbow—anteroposterior and lateral—usually suffice for evaluation of these fractures.
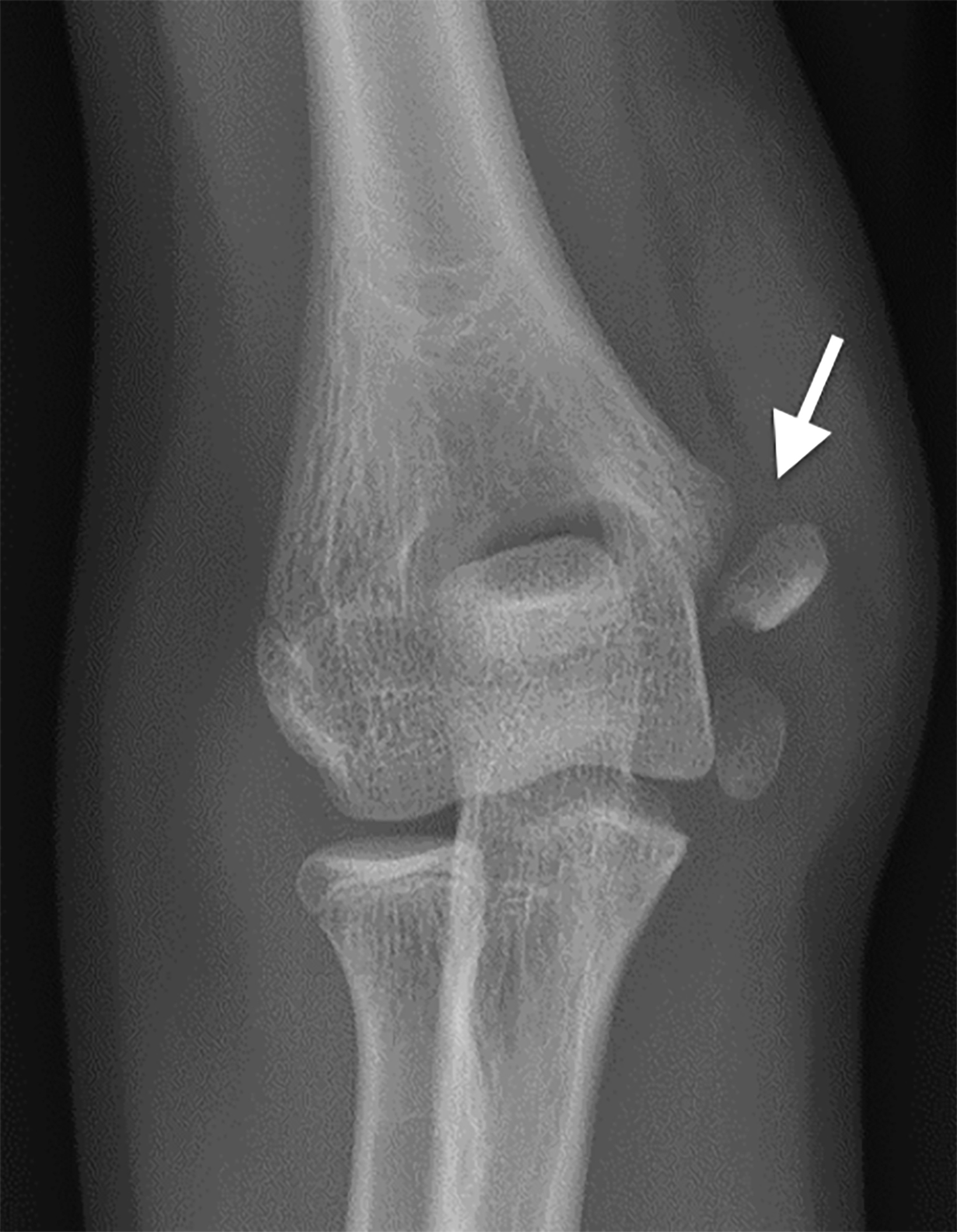
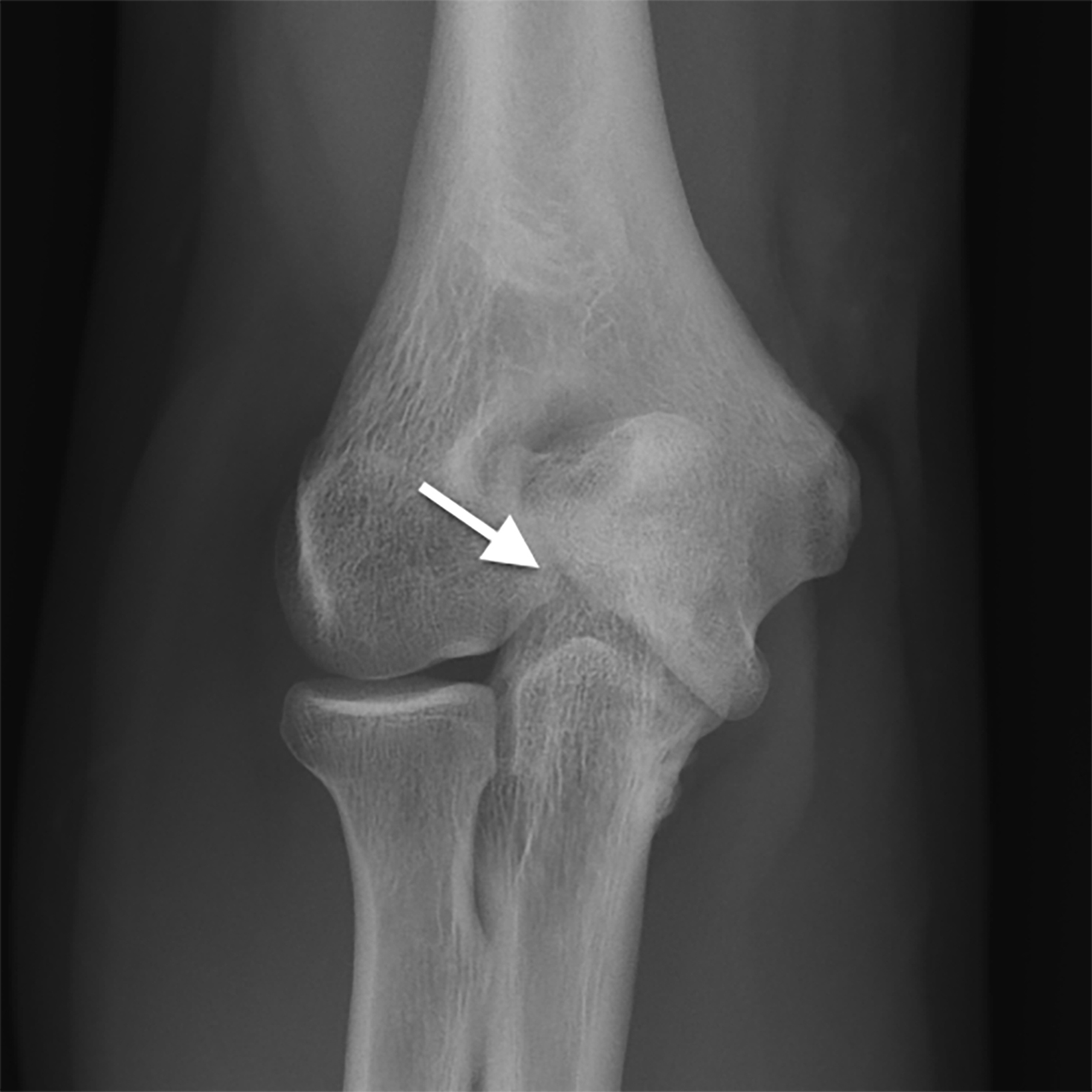
Medial epicondyle fractures account for up to 20% of cases. Their mechanism of injury consists of acute valgus stress associated with forearm flexor-pronator muscle contraction, from either overhead throwing or falling on an outstretched arm.7,8 Patients, typically 9 to 14 years of age, present with acute pain over the medial aspect of the elbow.7 Radiographs demonstrate a displaced medial epicondyle with physeal widening (Figure 4). The epicondyle may move into the joint space, resulting in “entrapment” (Figure 5). The entrapped medial epicondyle may be mistaken for a trochlea. Close inspection of the elbow joint is warranted if radiography does not reveal a medial epicondylar apophysis in a child older than 6 or 7 years. Minimally displaced fractures can be treated with rest and immobilization; surgery is required for severely displaced and entrapped fragments.7
Lateral condyle fractures usually occur in children 6 to 14 years of age and result from a varus force on an extended elbow with the forearm in supination. Radiographs show a fracture plane through the lateral condyle. They are most commonly considered Salter-Harris IV fractures, although they often appear on radiographs to be Salter-Harris II fractures. They are surgically managed when displaced by greater than 2 mm.
With respect to chronic elbow injuries, the term “Little League elbow” historically has referred to avulsion injuries of the medial epicondyle, but it has been applied more recently to describe injuries at other elbow sites.8,9 These include the lateral articular surface (capitellum), posterior articular surface (olecranon), and trochlea.9 Children participating in sports that entail overhead throwing are at higher risk for these injuries, several types of which are described below.
Medial Compartment Injuries
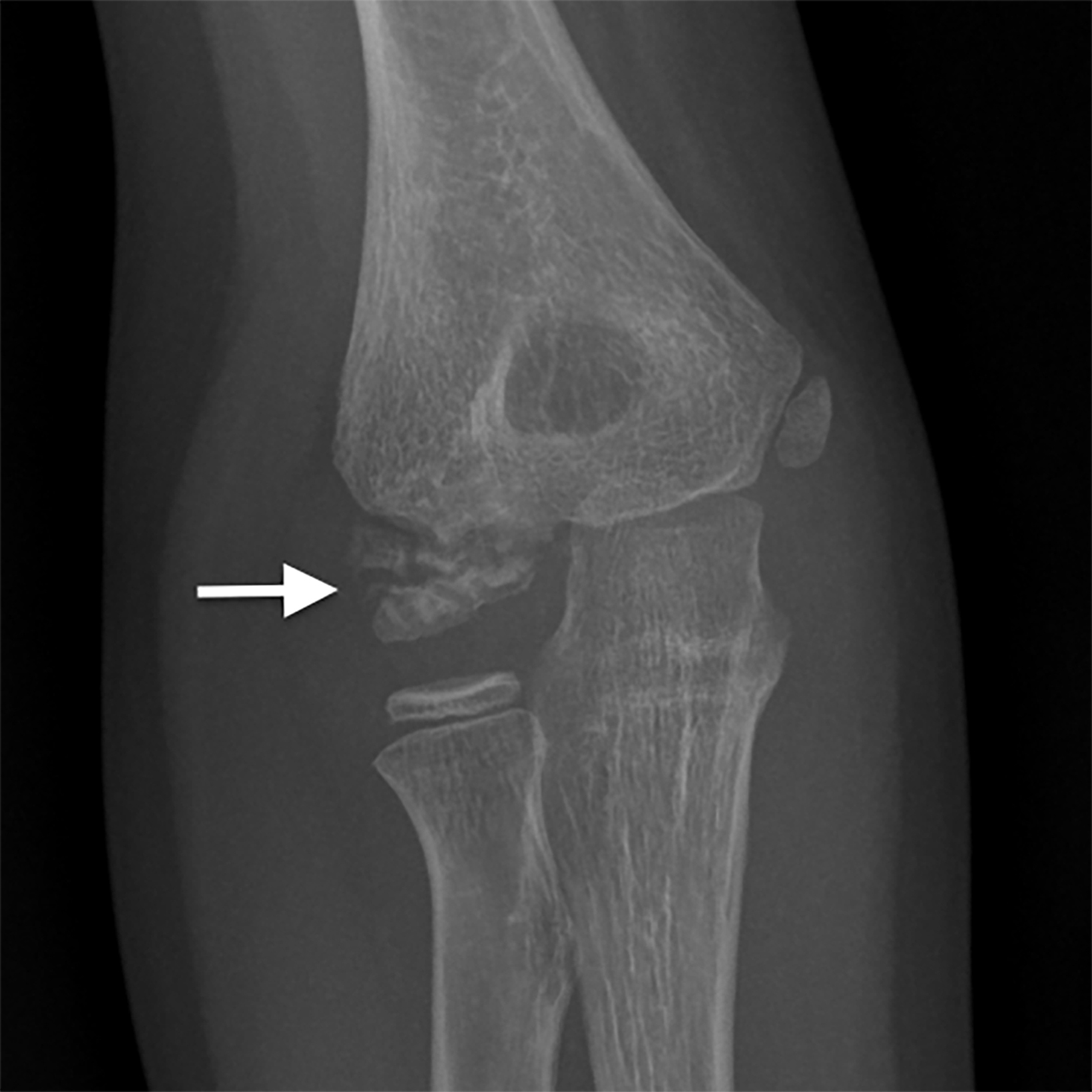
Medial epicondylar apophysitis is the most common repetitive elbow injury. The underlying mechanism is recurrent valgus stress during the acceleration phase of throwing, which leads to traction apophysitis. Patients are typically 11 to 12 years of age and present with medial elbow pain and tenderness. Radiographic findings include widening of the medial epicondyle physis, representing a chronic Salter-Harris I fracture from physeal microtrauma, and irregularity and sclerosis of the apophysis (Figure 6).2,9 MRI is more sensitive than radiography for diagnosis; findings consist of physeal widening and increased signal intensity in the epicondyle apophysis, representing marrow edema.8 Nonunion may result if the lesion is left untreated, but the prognosis is good with joint rest.
Lateral Compartment Injuries
Typically involving the capitellum, lateral compartment injuries include Panner disease and osteochondritis dessicans. They affect different age groups and generally occur in athletes engaged in overhead throwing.1,2,10 Their mechanism of injury is repetitive lateral compressive forces on the developing capitellum. Symptoms include several weeks of pain and stiffness. Although plain radiographs may demonstrate the lesion, MRI is more sensitive in diagnosing and showing their extent, which can impact management.
Panner disease is a self-limiting osteochondrosis of the capitellar ossification center. Affected athletes are typically younger than 10 years.8 Radiographs show flattening, sclerosis, and fragmentation of the capitellar epiphysis, with involvement of the entire capitellar ossification center. MRI reveals decreased T1- and increased T2-signal intensity, representing diffuse edema (Figure 7).8 The overlying cartilaginous surface is unaffected and osteochondral loose body formation does not occur. Treatment consists of immobilization, and the prognosis is excellent, with no residual deformity in most cases.
Osteochondritis dissecans, which typically affects patients older than 11 years, is a disorder in which a segment of articular cartilage separates from the subchondral bone.1,2,10 Unlike Panner disease, which involves the entire capitellar epiphysis, this lesion is usually localized to the anterolateral aspect of the ossifying epiphysis. Radiographic findings range from capitellar lucency and flattening in early disease, to capitellar fragmentation and loose bodies in late disease. MRI is the study of choice for confirming the diagnosis and differentiating between stable and unstable lesions. Both types show low T1 and variable T2 subchondral signal intensity. Findings of instability include a rim of high T2 signal intensity between the lesion and the subchondral bone, changes in the overlying cartilage, subchondral bone disruption, and intraarticular bodies(Figure 8).8 Stable lesions are managed with elbow rest, while unstable lesions may require arthroscopic intervention.2,8,10
Posterior Compartment Injuries
Stress injuries of the posterior elbow are relatively uncommon; they usually result from repetitive contraction of the triceps tendon during overhead throwing, leading to traction apophysitis of the olecranon. Radiographic findings are similar to those of medial epicondyle apophysitis and include physeal widening and sclerosis of the olecranon apophysis. MRI findings include physeal widening and abnormally high signal in the olecranon apophysis, representing periphyseal edema (Figure 9). There may also be associated edema in the triceps tendon. The prognosis is good with rest and suspension of throwing.
Trochlear Injuries
Trochlear injuries, typically seen in adolescents, result from overhead throwing motion. They include osteochondritis dissecans and fishtail deformity of the distal humerus, both of which can present with chronic elbow pain and limited motion.8,11 Radiographic findings of osteochondritis dissecans mimic those of capitellar osteochondritis and include subchondral lucency, sclerosis and fragmentation in the lateral aspect of the trochlea, and loose body formation.8,11 Lesion stability can be assessed with MRI, and they can be treated similarly to capitellar osteochondritis.
Fishtail deformity of the distal humerus, a late complication of distal humeral fractures, is uncommon. This injury is thought to result from post-traumatic avascular necrosis of the trochlear cartilage.12 Clinical findings include limited motion, stiffness, and pain related to associated synovitis, osteoarthritis, loose bodies, and cubitus valgus deformity.
Radiographs show a wedge-shaped or concave defect in the distal humerus with elongation and underdevelopment of the lateral trochlea, giving rise to a fishtail or chevron-like deformity (Figure 10). Additional findings include changes of osteoarthritis ( joint space narrowing, osteophyte formation, and subchondral cystic changes), migration of the ulna, and radial subluxation.12 MR imaging can be useful to determine the extent of osseous and cartilaginous abnormalities (Figure 10). Treatment includes rest and arthroscopic debridement.
Acute and Chronic Injuries of the Wrist and Fingers
Buckle, complete, and SalterHarris fractures of the distal radial metaphysis are common acute wrist fractures in pediatric athletes. They typically occur from a fall on a hyperextended wrist; skaters and soccer players are at a higher risk for these injuries. Distal radial fractures typically heal with immobilization. The scaphoid is the most commonly injured carpal bone.2 Mechanisms of injury include a direct blow or a fall on an outstretched hand. Fractures occur most frequently in the scaphoid waist and less often in the proximal or distal poles (Figure 11).13 Casting results in a 90% union rate.
Stress injuries of the distal radial physis, often referred to as “gymnast wrist,” are common chronic injuries among gymnasts and weightlifters between 12 and 14 years of age. The mechanism of injury is repetitive trauma to the distal radius in wrist extension.1 Radiographs show distal radial physeal widening, corresponding to a Salter-Harris I fracture, and associated metaphyseal irregularity and sclerosis (Figure 12). Prognosis is good with immobilization, but continued repetitive stress may cause bridging or a bony bar and premature closure of the distal radial physis, resulting in relative ulnar lengthening. MR imaging is preferred for evaluating physeal bridging or a bony bar.
Repetitive phalangeal flexion and extension in rock climbing can cause Salter-Harris II or III fractures of the bases of the middle phalanges of the third or fourth digits.1,4
Conclusion
Sports injuries in young athletes typically involve the cartilaginous physes of the shoulder, elbow, and wrist, which are the weakest parts of the musculoskeletal system. Conventional radiography is the modality of choice for diagnosing most of these injuries, but MRI can be valuable in diagnosing subtle lesions and assessing signs of instability in osteochondral defects.
References
- Delgado J, Jaramillo D, Chauvin NA. Imaging the injured pediatric athlete: upper extremity. Radiographics. 2016; 36:1672–1687.
- Emery KH. Imaging of sports injuries of the upper extremity in children. Clin Sports Med. 2006; 25:543–568.
- Lomasney LM, Lim-Dunham JE, Cappello T, Annes J. Imaging of the pediatric athlete: use and overuse. Radiol Clin North Am. 2013; 51:215–226.
- Paz DA, Chang GH, Yetto MJ, et al. Upper extremity overuse injuries in pediatric athletes: clinical presentation, imaging findings and treatment. Clin Imaging. 2015; 39:954–964.
- Cross GWV, Reilly P, Khanna M. Salter-Harris Type I coracoid process fracture in a rugby playing adolescent. BJR Case Rep. 2018:20180011.
- Carson WG, Gasser SI. Little Leaguer’s Shoulder. A report of 23 cases. Am J Sports Med. 1998;26:575–580.
- Gottschalk HP, Eisner E, Hosalkar HS. Medial epicondyle fractures in the pediatric population. J Am Acad Orthop Surg. 2012;20:223–232.
- Wong TT, Lin DJ, Ayyala RS, Kazam JK. Elbow injuries in pediatric overhead athletes. AJR. 2017: 209:849–859.S
- Dwek JR, Chung CB. A systematic method for evaluation of pediatric sports injuries of the elbow. Pediatr Radiol. 2013;43:120–128.
- Van Bergen CJA, Van den Ende KIM, Brinke BT, Eygendaal D. Osteochondritis dissecans of the capitellum in adolescents. WJO. 2016;7:102–108
- Marshall KW, Marshall DL, Busch MT, Williams JP. Osteochondral lesions of the humeral trochlea in the young athlete. Skeletal Radiol. 2009;38:479–941.
- Narayanhan S Shailam R, Grottkau BE, Nimkin K. Fishtail deformity – a delayed complication of distal humeral fractures in children. Pediatr Radiol. 2015; 45:814–819.
- Gholson JJ, Bae DS, Zurakowski D, Waters PM. Scaphoid fractures in children and adolescents: contemporary injury patterns and factors influencing time to union. J Bone Joint Surg AM. 2011; 93:1210–1219.
References
Citation
JR W, G S, MJ S. Imaging Upper Extremity Injuries in Pediatric Athletes. Appl Radiol. 2022;(2):7-14.
March 4, 2022