Epidural Lipomatosis
Images


Case Summary
An adult with a history of type II diabetes mellitus, hypothyroidism, COPD, asthma, and cervical cancer presented with lower back pain exacerbated by walking and relieved with rest. The patient described the pain as 7/10 and associated with numbness and tingling that radiated down both legs but was more pronounced in the right leg. Physical examination revealed tenderness to palpation of the lumbar paraspinal musculature with muscle spasms. Pain was elicited with 60 degrees of flexion of the hips bilaterally. There was decreased sensation to light touch in the right lower extremity in an L3-L5 dermatomal distribution. Patellar reflexes were 1+ bilaterally.
Imaging Findings
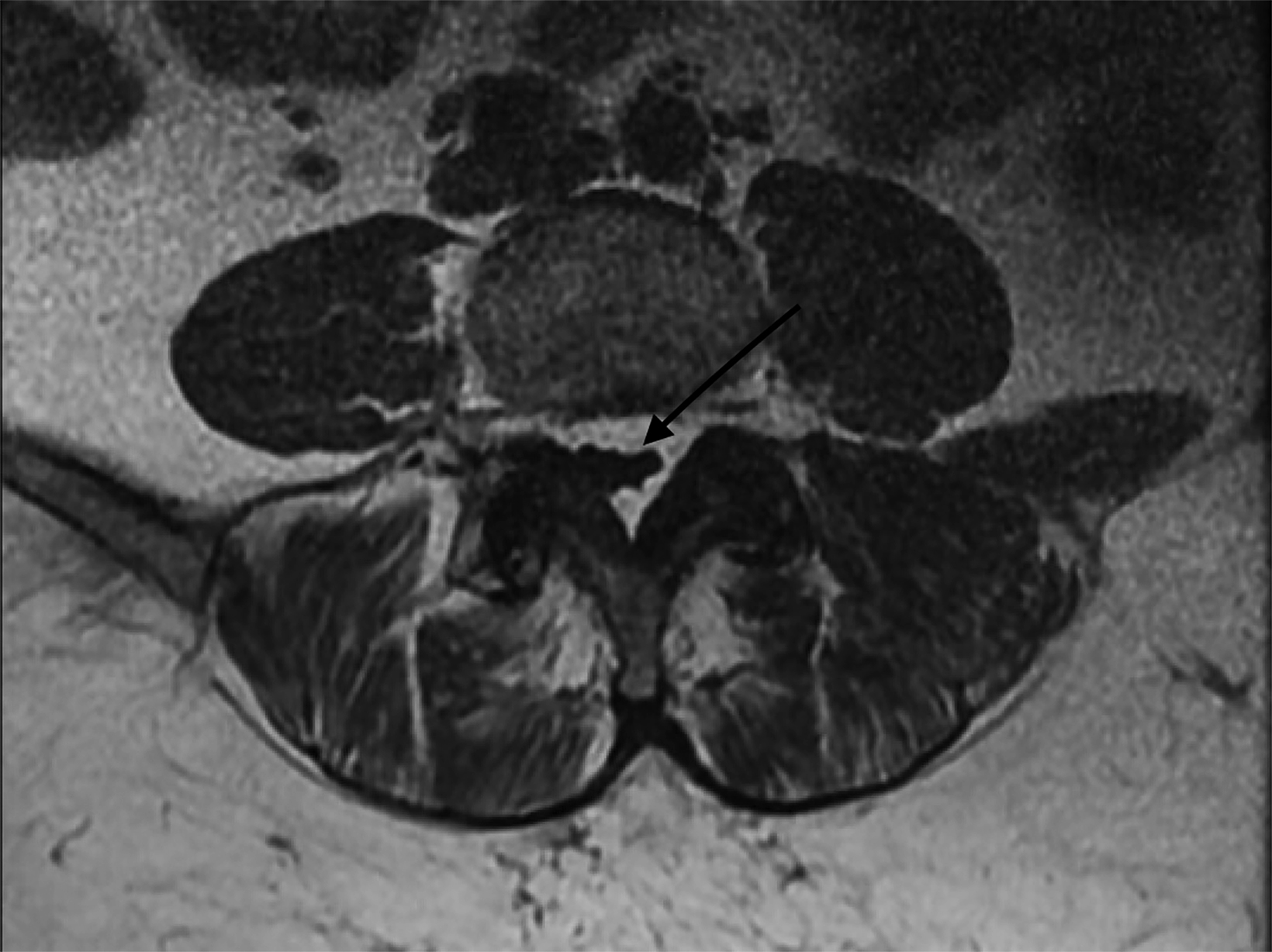
Magnetic resonance imaging of the lumbosacral spine (Figures 1,2) demonstrated prominent epidural fat surrounding the thecal sac, from approximately the L3 level and inferiorly. Axial images, particularly at the L4-L5 level (Figure 3), revealed the fat causing deformation and significant stenosis of the thecal sac. The polygonal deformation of the dural sac was a pathognomonic sign of the condition.
Diagnosis
Epidural lipomatosis. Clinical differential diagnoses for typical symptoms include herniated disc, narrowing of the spinal canal, spondylolysthesis, and distal polyneuropathy.
Discussion
Spinal epidural lipomatosis is caused by an overgrowth of adipose tissue in the epidural space. This leads to narrowing of the spinal canal and compression of neural structures.1 Patients may be asymptomatic in the early stages of disease. However, with progression and compression of different regions of the spinal canal, patients may present with back pain, weakness, paresthesias, claudication, radiculopathy, sensory disturbances, and/or ataxia.2
Epidural lipomatosis is most often associated with exogenous steroid use. It is less common in patients without steroid use secondary to obesity or endogenous steroid excess. It may also be idiopathic. Men are more commonly affected than women.3
The most sensitive test for the condition is MRI, particularly T1 where the fat will be white. The pathognomonic “Y” shape polygonal deformation of the dural sac is caused by compression due to excess fat.2 The “Y” sign does not become apparent until the disease is severe. Grading of epidural lipomatosis (I, II, III) is based on the epidural fat-to-spinal-column index, with normal values being less than 40%. The condition is designated as Grade III when the “Y” sign is first seen on MRI and the epidural fat-to-spinal-column ratio is greater than 75%.4
Epidural lipomatosis can be managed with steroid taper and discontinuation or with laminectomy and epidural fat resection. Approximately 90% of cases are managed surgically, which is considered in severe cases or where conservative treatment has failed.5 Weight reduction strategies can be beneficial in alleviating patients with epidural lipomatosis secondary to obesity.6 Clinical trials have not been conducted to compare outcomes of conservative and surgically managed cases.2
Conclusion
Epidural lipomatosis has the potential to cause spinal stenosis, which can be diagnosed with MRI. Imaging determines extent to which epidural lipomatosis has affected the spinal canal and can facilitate surgical planning.
References
- Kim K, Mendelis J, Cho W. Spinal epidural lipomatosis: a review of pathogenesis, characteristics, clinical presentation, and management. Global Spine J. 2019; 9(6):658-665. doi: 10.1177/2192568218793617. Epub 2018 Aug 13. PMID: 31448201; PMCID: PMC6693071.
- Walker PB, Sark C, Brennan G, Smith T, Sherman WF, Kaye AD. Spinal epidural lipomatosis: a comprehensive review. Orthop Rev (Pavia). 2021;13(2): 25571.doi: 10.52965/001c.25571. PMID: 34745483; PMCID: PMC8567763.
- Lévy-Weil FE, Feldmann JL. Lipomatose épidurale [Epidural lipomatosis]. Presse Med. 2000; 29(9): 469-475. French. PMID: 10745936.
- Borré DG, Borré GE, Aude F, Palmieri GN. Lumbosacral epidural lipomatosis: MRI grading. Eur Radiol. 2003; 13(7):1709-1721. doi: 10.1007/s00330-002-1716-4. Epub 2002 Dec 13. PMID: 12835988.
- Koch CA, Doppman JL, Patronas NJ, Nieman LK, Chrousos GP. Do glucocorticoids cause spinal epidural lipomatosis? When endocrinology and spinal surgery meet. Trends Endocrinol Metab. 2000; 11(3):86-90. doi:10.1016/s1043-2760(00)00236-8. PMID: 10707048.
- Kniprath K, Farooque M. Drastic weight reduction decrease in epidural fat and concomitant improvement of neurogenic claudicatory symptoms of spinal epidural lipomatosis. Pain Med. 2017;18(6):1204-1206. doi:10.1093/pm/pnw313. PMID: 28108643.
Citation
F S, M W, S L. Epidural Lipomatosis. Appl Radiol. 2024;(1):48j-48k.
January 24, 2024