DL-Based, Rapid FFR-CT Algorithm Facilitates Clinical Adoption
Images
A high-speed onsite deep-learning based fractional flow reserve (FFR)-CT algorithm yielded excellent diagnostic performance for the presence of hemodynamically significant stenosis, with both high interobserver and intraobserver reproducibility. That’s according to a published study in the American Journal of Roentgenology.
“A rapid and accurate onsite approach for determining FFR-CT should address challenges encountered in the clinical adoption of prior FFR-CT implementations,” wrote corresponding author Ronny Ralf Buechel, MD, from University Hospital Zurich in Switzerland.
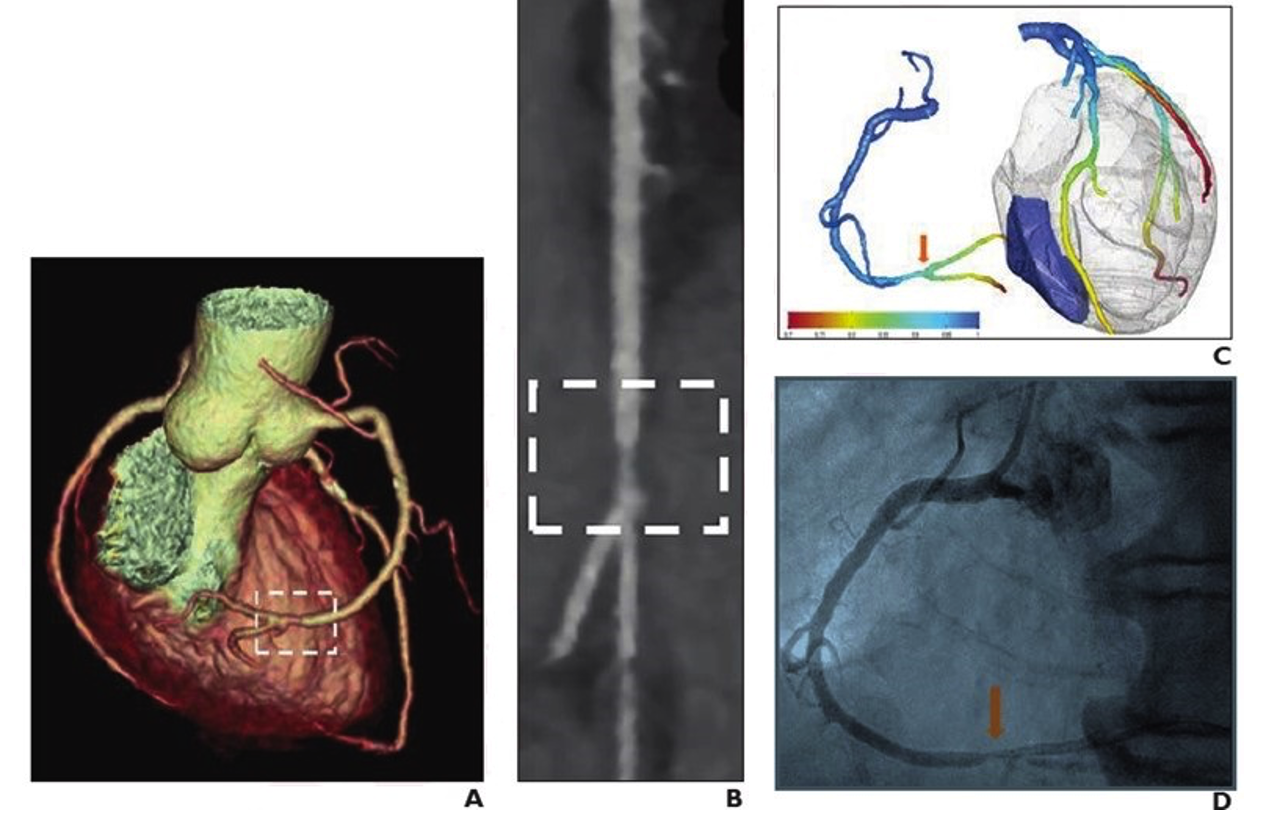
In the study, 59 patients (46 men, 13 women; mean age 66.5 years) underwent coronary CTA (including calcium scoring) followed within 90 days by invasive angiography with invasive FFR and/or instantaneous wave-free ratio (iwFR) measurements from December 2014 to October 2021. Coronary artery lesions were considered to show hemodynamically significant stenosis in the presence of invasive FFR ≤0.80 and/or iwFR ≤0.89. A single cardiologist evaluated CTA images using an onsite deep-learning based semiautomated algorithm employing a 3D computational flow dynamics model to determine FFR-CT for coronary artery lesions detected by invasive angiography. Then, time for FFR-CT analysis was recorded. FFR-CT analysis was repeated by the same cardiologist in 26 randomly selected examinations, as well as by a different cardiologist in 45 randomly selected examinations.
Ultimately, Buechel et al.’s onsite deep-learning based FFR-CT algorithm evidenced AUC for hemodynamically significant stenosis—based on invasive angiography—of 0.975, sensitivity of 93.5%, and specificity of 97.7%. Among severely calcified lesions, their same algorithm had AUC of 0.991, sensitivity of 94.7%, and specificity of 95.0%. Moreover, the mean analysis time was 7 minutes and 54 seconds.
“To our knowledge, the currently reported mean processing timer represents the fastest reported time for onsite FFR-CT analysis,” the authors concluded.