Complete sagittal duplication of the urinary bladder






Complete duplication of the urinary bladder. Differential diagnosis: incomplete duplication of the urinary bladder, urinary bladder diverticulum and cloacal malformation.
Findings
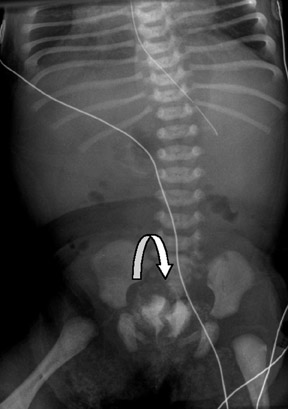
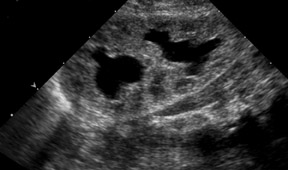
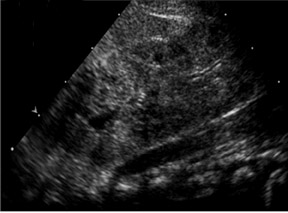
The VCUG (Figures 1 and 2) demonstrated a complete duplication of the urinary bladder. Abdominal ultrasound (Figure 3) showed moderate left hydronephrosis without ureteral dilatation.
Discussion
Complete duplication of the urinary bladder is a rare anomaly with only about 50 reported cases. Urinary bladder anomalies are generally diagnosed in infancy or childhood when causes of urinary tract infections are evaluated.1
The cause of complete duplication of the urinary bladder remains obscure, although a few hypotheses have been proposed. Abrahamson2 offers 2 explanations:
- Excessive constriction between the urogenital and vesicourethral portions of the ventral cloaca.
- A supernumerary cloacal septum that indents the epithelial of the urinary bladder.
Disturbances in the embryogenesis of the hindgut may result in duplication of the lower urinary tract.3 The primitive hindgut is the anlage of the terminal ileum, colon and cloaca. The cloaca is divided into anterior and posterior positions which form the lower genitourinary and lower gastrointestinal systems, respectively.
Early embryologic duplication of the hindgut could cause complete duplication of the 2 systems.1,3
Duplication of the urinary bladder may occur in the sagittal or coronal plane. The most common form is sagittal duplication, in which 2 urinary bladders lie side by side and are separated by a fold of peritoneum and loose areolar tissue. Each urinary bladder receives the ureter of the ipsilateral kidney and is drained by its own urethra, with the ureter and urethra lying side by side.4,5
In some cases, only 1 bladder communicates with a single urethra, leaving the opposite side obstructed with no outlet.6,7 Most obstructed systems are associated with renal dysplasia and are nonfunctional.
Complete duplication of the urinary bladder in the coronal plane is much more unusual. In this anomaly, the 2 urinary bladders lie one in front of the other and are separated by a fibromuscular septum that runs obliquely in a posterosuperior to anteroinferior plane. Each urethra originates from a separate urinary bladder.
Associated congenital anomalies include some type of duplication of the external genitalia; duplication of the vagina and urethra have also been reported, as well as duplication of the lower gastrointestinal tract and fistulas between the rectum, vagina and urethra.
Conclusion
Complete duplication of the urinary bladder is rare, with <50 reported cases. Duplication can be complete or partial, although the complete urinary bladder duplication more common. Duplication may occur in the sagittal (more common) or coronal planes, with the corresponding ipsilateral ureter draining each half of the urinary bladder. In most cases there is associated duplication of the urethra, but in a few cases, only 1 bladder communicates with a single urethra, leaving the opposite side obstructed with no outlet.
Associated abnormalities with complete duplication of the urinary bladder include duplication of the penis, vagina, uterus, lumbar vertebrae and hindgut. In addition, there may be fistulous connection between the rectum, vagina and urethra.
Surgical correction is usually indicated for the associated congenital external genitalia and lower gastrointestinal tract anomalies.
The prognosis is good. Yearly renal ultrasound evaluation as clinically indicated is recommended to evaluate potential complications of urinary tract infections or urinary bladder calculus.
- Esham W, Holt HA. Complete duplication of bladder and urethra: A case report. J Urol. 1980; 123:773-775.
- Abrahamson J. Double bladder and related anomalies: Clinical and embryological aspects and a case report. Br J Urol. 1961; 33:195-198.
- Okur H, Keskin E, Zorludemir U, Olcay I. Tubular duplication of the hindgut with genitourinary anomalies. J Pediatric Surg. 1992; 27:1239-1240.
- Hoffman AD, Leroy AJ. Uroradiology: Procedures and anatomy. In Kelalis PP, King LR, Belman AB, eds. Clinical pediatric urology. 3rd ed. Philadelphia, PA. Saunders;1992:66-116.
- Moore KL. The urogenital system. In: Moore KL, eds. The developing human: Clinically oriented embryology. 3rd ed. Philadelphia, PA. Saunders;1982:255-297.
- Dunetz GN, Bauer SB. Complete duplication of bladder and urethra. Urology. 1985; 25:179-182.
- Cheng EY, Maizels M. Complete duplication of the bladder in the coronal plane: Case report. J Urol. 1996;155:1414-1415.