Atrial Fibrillation Patients Benefit from 4D Flow MRI and 3D Printed Phantoms
Images
A Summa Cum Laude award-winning scientific paper presented at ARRS 2023 indicates that correctly occluded left atrial appendages (LAAs) could present maximal reduction in left atrial (LA) flow stasis and thrombogenicity, offering a clinical goal for the procedure in patients with atrial fibrillation.
Pointing out the paucity of knowledge in atrial fibrillation (AF) populations regarding the actual flow dynamic changes before and after percutaneous left atrial appendage occlusion (LAAO), “we aimed to evaluate LA flow dynamics for pre-occluded, correctly occluded, and incorrectly occluded LAAs in patients with AF via four-dimensional (4D) flow MRI and 3D printed phantoms,” said Min Jae Cha from the department of radiology at Chung-Ang University Hospital in Seoul, South Korea.
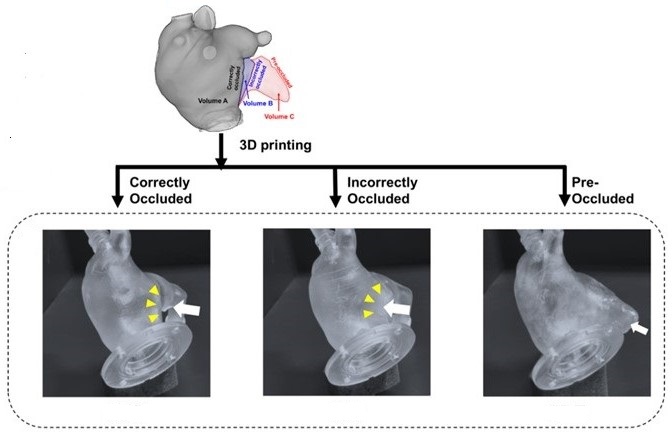
In the paper, life-sized LA phantoms of an 86-year-old patient with persistent AF were 3D printed from cardiac CT images. Setting a custom-made, closed-loop flow circuit, a pump delivered pulsatile pulmonary venous flow. Using a 3T scanner (Philips Achieva TX), 4D flow MRI was obtained, then analyzed via MATLAB-based software. Flow metrics associated with blood stasis and thrombogenicity—stasis volume defined by velocity threshold (|V| < 3 cm/s), time-averaged wall shear stress (WSS), and endothelial cell activation potential (ECAP)—were compared among three conditions.
According to Cha et al., different spatial distributions, orientations, and magnitudes of flow were directly visualized within the three LA phantoms using 4D flow MRI. The time-averaged volume and percentage of LA flow stasis were consistently minimized in the correctly occluded model (70.82 ml, 38.97%), followed by the incorrectly occluded (73.17 ml, 39.02%) and pre-procedural (79.11 ml, 39.71%) models.
Additionally, the pre-occluded model was associated with the lowest surface-and-time-averaged WSS (0.048 Pa), followed by incorrectly (0.059 Pa) and correctly (0.072 Pa) occluded models. Conversely, ECAP was lowest in the correctly occluded model (4.004 Pa-1), followed by the incorrectly- (4.792 Pa-1) and pre-occluded (5.861 Pa-1) models.