Arrested Pneumatization of the Left Central Skull Base
Images
Case Summary
An adult with a history of headache and obstructive sleep apnea presented to their primary care provider with nasal congestion. The patient had no other relevant medical history of chronic illness. The patient also had no history of smoking and was not on blood thinners.
Imaging Findings
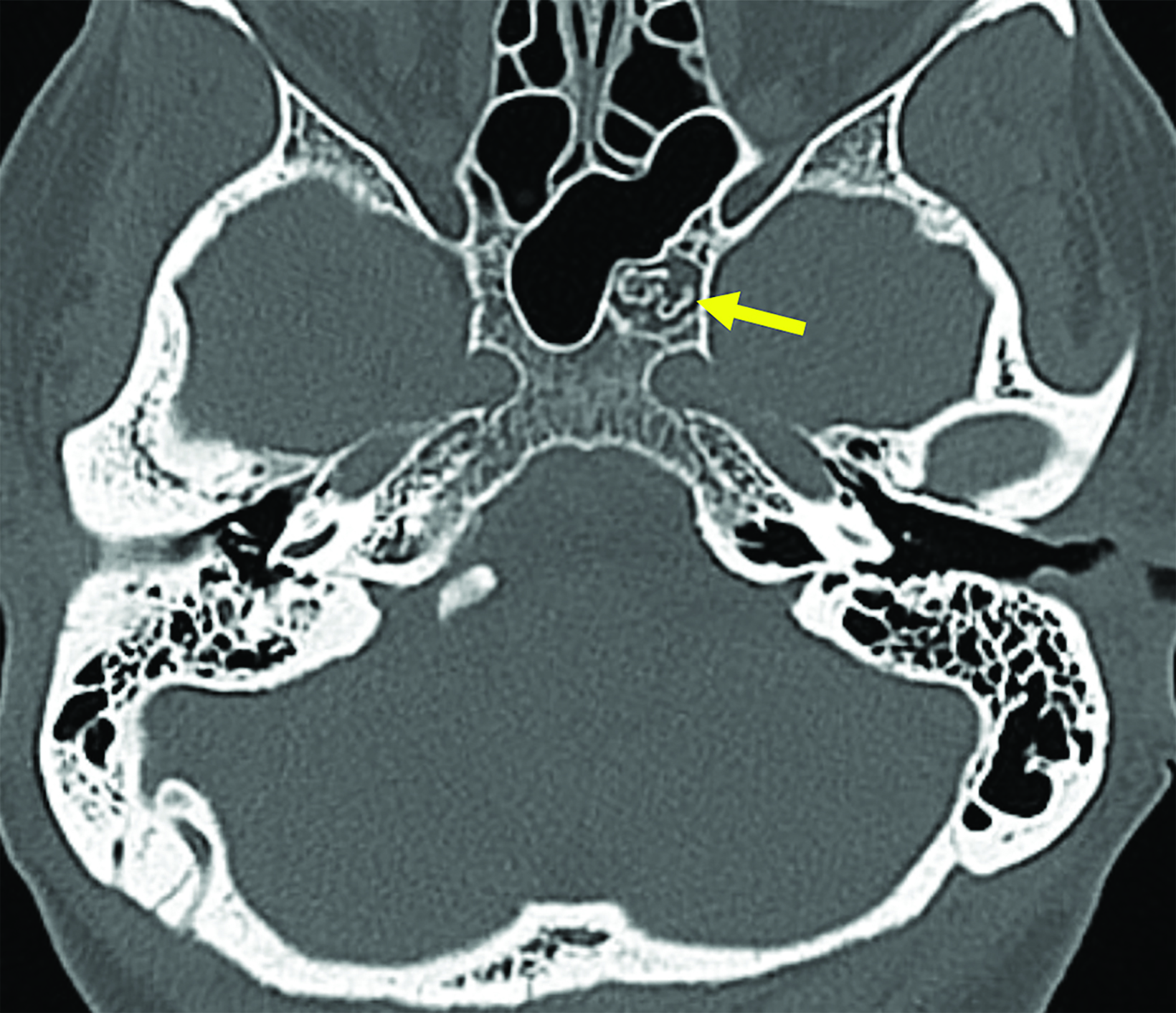
Maxillofacial CT scan (Figure 1) revealed a nonexpansile lesion involving the left central skull base. Further examination revealed internal curvilinear calcifications with well-defined sclerotic margins.
Diagnosis
Arrested pneumatization of the left central skull base
Discussion
Arrested pneumatization (AP) is a commonly misdiagnosed condition that occurs in the early stages of fetal development and continues through childhood and puberty.1 Sinus development diverges from the typical developmental pattern.2 Arrested pneumatization results from the failure of pneumatization before respiratory mucosa can extend into locations of early fatty marrow conversion.2 This uncommon developmental variant typically occurs near the sphenoid sinus in the central skull base. The etiology for this maldevelopment is currently unknown, and diagnosis is usually incidental on imaging for another condition. Some potential factors that may contribute to this entity include bone composition and vascularization, although further research is necessary.1
Preoperative diagnosis with CT and MRI is key to avoiding unnecessary surgery and/or other treatment of AP, which is widely considered a normal variant in fetal development that requires no additional treatment. A specific set of four criteria must be met for confident diagnosis: 1) the lesion must be located at a site of normal pneumatization or accessory sphenoid sinus pneumatization; 2) the lesion should have thin, well-defined sclerotic margins; 3) the lesion must be nonexpansile; and 4) internal curvilinear calcifications must be present.2-4
Detailed inspection of images, coupled with awareness of the entity, can aid in making the diagnosis.1 Mistaking this entity can contribute to unnecessary surgeries and/or follow-up examinations. Possible differential considerations include but are not limited to ossifying fibroma, bone metastases, and chondrosarcoma.2
Conclusion
Arrested pneumatization is a developmental variant with a poorly understood etiology. Radiologists should be familiar with the key features of AP on CT and MRI in order to make an accurate diagnosis.
References
- Park S-H, Hwang J-H. Arrested pneumatization of the sphenoid sinus in the skull base. Brain Tumor Research and Treatment. 2021; 9 (1):40-43. doi:10.14791/btrt.2021.9.e2
- Welker KM, DeLone DR, Lane JI, Gilbertson JR. Arrested pneumatization of the skull base: Imaging characteristics. Am J Roentgenol. 2008;190 (6):1691-1696. doi:10.2214/ajr.07.3131
- Duignan M, Wood A. Arrested pneumatization of the skull base: An under-recognized skull base anomaly. ANZ J Surg.. 2020; 91(1-2). doi:10.1111/ans.16118
- Jalali E, Tadinada A. Arrested pneumatization of the sphenoid sinus mimicking intraosseous lesions of the skull base. Imaging Sci Dentistry. 2015; 45 (1):67-72. doi:10.5624/isd.2015.45.1.67
Citation
V R, D R, S R. Arrested Pneumatization of the Left Central Skull Base. Appl Radiol. 2024;(2):45.
March 5, 2024