Sonographic mammographic correlation




Dr. Lucas-Fehm is a Clinical Assistant Professor of Radiology, Thomas Jefferson University Hospital, Breast Imaging Center, Philadelphia, PA.
Ultrasound plays a vital role in the assessment of breast masses. Its primary use has been for the differentiation of solid from cystic masses and as guidance for interventional procedures. However, in recent years, ultrasound as an adjunct to mammography has improved accuracy in the diagnosis of breast cancer. 1 Certain ultrasound features can help differentiate benign from malignant mass- 2,3 In solid masses, evaluation of the shape, margins and width-to-anteroposterior (AP) ratio can be useful in avoiding unnecessary excisional biopsy. 2 Assessment of the walls of cystic lesions, as well as the presence of septations and intracystic masses, is important in determining whether a biopsy is warranted. 3 In the evaluation of asymmetric densities seen at mammography, the presence of an ultrasound abnormality can raise the index of suspicion for malignancy. 4 As it has become more widely utilized, studies have shown that the most beneficial role of ultrasound may lie in the evaluation of a mammographic mass that is partially obscured or in dense breast tissue where mammography is unable to fully characterize or detect a lesion. 2,5-7
Evaluation of breast masses
Sickles described the systematic approach for evaluation of a mammographically detected mass. 8 Size, location, density, shape, clarity of margins, and interval change from prior studies are factors to be evaluated when analyzing mammographic masses. 8
A method for the analysis of sonographic masses was described by Rahbar et al. 2 The authors reported that sonographic features that most reliably indicate if a mass is benign are a round or oval shape, circumscribed margins, and a width-to-AP dimension ratio >1.4. Masses with an irregular shape, microlobulations, spiculations, and a width-to-AP dimension ratio ≤1.4 are more likely to be malignant. 2
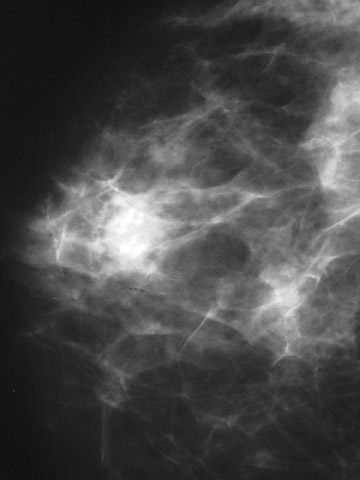
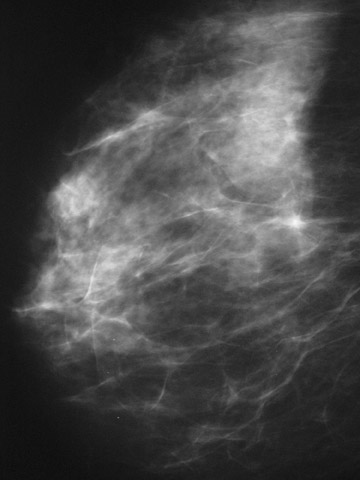
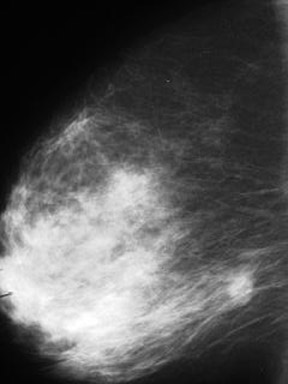
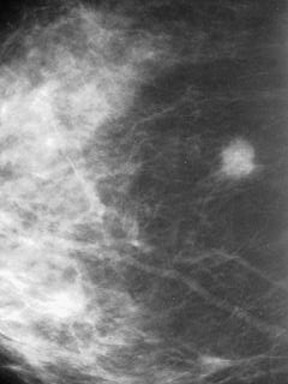
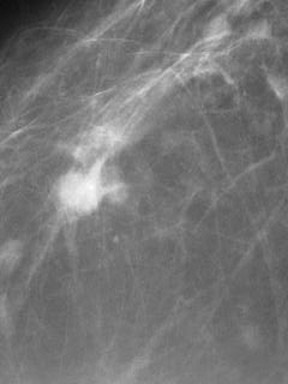
It can be concluded from these studies that the evaluation of the shape and margins are the most important factors in the mammographic and sonographic assessment of masses (Figures 1 and 2).
Improvement in diagnostic accuracy with ultrasound
Ultrasound utilized as an adjunct to mammography increases diagnostic accuracy. 1 Zonderland et al 1 performed a 2-year prospective study in which 4811 mammograms were evaluated and classified into one of the following 5 categories:
Level 1- Benign with no abnormalities seen.
Level 2- A lesion or cluster of microcalcifications with a high probability of being benign.
Level 3- Equivocal with a lesion or microcalcifications that are indeterminate, requiring histopathologic examination.
Level 4- Probably malignant with a lesion or microcalcifications that arouse suspicion of malignancy.
Level 5- Malignant when a highly suspicious lesion was present in combination with associated features of malignancy.
Ultrasound was then performed on possible cysts, palpable abnormalities, and mammographically detected lesions. Of the 4811 mammograms evaluated, 1103 were followed by ultrasound. The ultrasounds were then categorized as follows: Benign- A simple cyst was considered benign. Probably benign- A cystic lesion with debris-like contents was considered probably benign. A solid lesion with smooth or lobulated margins
that was sharply defined, with homogeneous hypoechoic contents and a horizontal orientation was assumed to be a fibroadenoma and classified as probably benign. Equivocal- A complex cyst with internal echoes and septa was classified as equivocal. Solid, hypoechoic lesions with irregular margins and an indeterminate or horizontal orientation but without a definite probability of being malignant or benign were considered equivocal. Probably malignant- A thickened wall and the presence of an intracystic mass were classified as probably malignant. Hypoechoic lesions with irregular and poorly defined margins with shadowing and vertical orientation were placed in this category.
Malignant- Lesions with infiltration into the surrounding fatty tissue or other associated features of malignancy.
Definitive diagnoses were then obtained for all 4811 cases after a mean follow-up of 30 months. The results showed that mammography identified 282 of 338 breast cancers. An additional 25 cancers were diagnosed with ultrasound. Ultrasound, therefore, increased the sensitivity by 7.4%.
A closer look at the 25 additional cancers diagnosed with ultrasound reveals that for 12 patients, the lesion was not recognized on the mammograms and even following retrospective review, 8 of the cancers remained occult. The other 13 cases had been characterized as probably benign on mammography but were reclassified and biopsied following ultrasound.
A review of the 13 cases that had been characterized as probably benign on mammography and then reclassified as suspicious on ultrasound reveals the need for ultrasound evaluation of masses seen at mammography. Two of the 13 cases were masses with well-defined margins on mammography. The level of suspicion was low and they were placed in the probably benign category. Subsequent ultrasound also found well-defined margins, but the presence of "debris-like contents" in the masses raised the level of suspicion, and biopsy yielded the diagnosis of intracystic papillary carcinomas. In the other 11 cases, the mammogram indicated a circumscribed lesion, a subtle architectural distortion, or an asymmetric density classified as probably benign. Follow-up ultrasound revealed characteristics raising the suspicion of malignancy.
These results show that ultrasound, when utilized as an adjunct to mammography, improves breast cancer detection with increased accuracy and characterization of lesions. In particular, it appears to be useful in the evaluation of asymmetric dense tissue seen at mammography.
Cystic lesions of the breast
Berg et al 3 identified 150 cystic lesions from a database of 2072 image-guided procedures. Lesions were placed into 7 categories: simple cyst; complicated cyst; cyst with thin septations; clustered microcysts; mass with thick wall and/or thick septations, intracystic mass, mixed cystic and solid; and solid mass with eccentric cystic foci.
No malignancies were found in the first 4 categories. Among these studies, 23 masses had thick, indistinct walls or thick septations and 7 of these were malignant. A total of 18 intracystic or mixed cystic and solid lesions were biopsied, and 4 proved to be malignant. Solid masses (n = 38) with eccentric foci were sampled, yielding 7 malignancies.
The authors concluded that cystic lesions with thick indistinct walls and/or thick septations, intracystic masses, and predominantly solid masses with eccentric cystic foci should be biopsied. Of the 79 complex masses in one of these 3 categories, 18 were malignant.
Focal asymmetric densities and ultrasound
Ultrasound plays a fundamental role in the workup of asymmetric breast tissue, densities seen in one projection, architectural distortion, and focal asymmetric densities. Samardar et al 4 discussed the usefulness of ultrasound when a mammogram detects a focal asymmetric density. Breast Imaging Reporting and Data System (BIRADS) categorizes 4 types of asymmetric breast findings: Asymmetric breast tissue; densities seen in one projection; architectural distortion; and focal asymmetric densities.
Additional mammographic imaging is the first means of evaluating asymmetric breast findings. Follow-up ultrasound evaluation should then be performed to search for a solid mass or focal shadowing that would raise suspicion for malignancy and warrant biopsy. Alternatively, ultrasound may find a cyst that would yield a benign diagnosis and warrant only routine follow-up.
Fat necrosis
Mammographic features of fat necrosis have been documented. They include radiographically lucent oil or lipid cysts, circumscribed water density masses, areas of increased density, pleomorphic clustered microcalcification, and suspicious spiculated masses. 9,10
Soo et al 9 described ultrasound findings associated with fat necrosis. The features varied, ranging from anechoic masses with posterior enhancement to solid masses. The authors placed their findings into 6 groups: Solid; complex with mural nodule; complex with echogenic band; anechoic with posterior acoustic enhancement; anechoic with acoustic shadowing; and no discrete mass.
Of the 31 masses identified by ultrasound, 29 had corresponding mammographic abnormalities. The remaining 2 masses were palpable with no mammographic findings. The masses were placed in one of the above-mentioned categories, and fat necrosis was diagnosed either by histology or on the basis of initial or follow-up mammographic findings.
Many of the sonographic features were nonspecific and could not be distinguished from findings of a malignant lesion. These included the masses placed in the category of a solid mass as well as those in the complex mass with a mural nodule group. Fat necrosis, which presents as an anechoic mass with acoustic enhancement, is indistinguishable from a cyst. However, the study did find that the indication of a complex mass with an echogenic band in patients with a trauma history should strongly suggest the diagnosis of fat necrosis. In these cases, aspiration or imaging follow-up should be considered in lieu of biopsy. Similarly, an anechoic mass with shadowing that corresponds to a mammographically benign lesion, such as an oil cyst, should be followed.
Doppler evaluation of breast masses
Power Doppler ultrasound is useful in detection of the pattern of distribution of blood vessels in breast masses. This is useful in the prediction of malignancy and is one more factor to be considered in the workup of breast lesions. 11,12
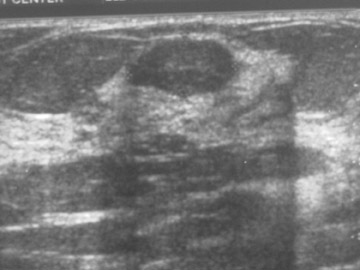
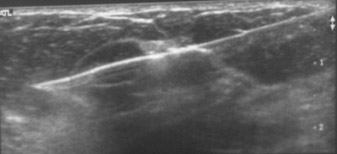
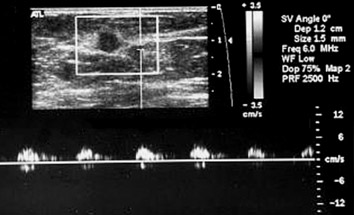
Raza and Baum 11 evaluated 86 solid breast masses that went on to biopsy. Grayscale and power Doppler ultrasound were utilized, and patterns of vascular distribution were assigned prior to biopsy. Vessels were categorized as penetrating, peripheral, central, or absent. Penetrating vessels were associated with malignancy. The results revealed that, using penetrating vessels to indicate malignancy, sensitivity for power Doppler ultrasound was 68%, specificity 95%, positive predictive value (PPV) 85%, and negative predictive value (NPV) 88% (Figure 3).
Dense breast tissue
Ultrasound is beneficial in dense breast tissue where the mammogram is unable to fully delineate or detect a lesion. Mammographic sensitivity for breast cancer declines with increasing breast density. 7,13 The American College of Radiology (ACR) defines 4 progressively more dense patterns in the BIRADS: 1) almost entirely fat; 2) scattered fibroglandular densities that could obscure a lesion; 3) heterogeneously dense, which may lower the sensitivity of mammography; and 4) extremely dense, which lowers the sensitivity of mammography. 14
In patients with BIRADS category 3 or 4 density breast tissue, bilateral whole-breast ultrasound is useful in detecting breast cancer not discovered with mammography or clinical examination. 5 A similar benefit has not been proven in BIRADS categories 1 or 2, in which mammography has a higher sensitivity. In short, the higher the sensitivity of mammography, the smaller the benefit of ultrasound. 1
Ultrasound of microcalcifications
Moon et al 15 prospectively studied 100 mammographically detected microcalcification clusters with ultrasound prior to biopsy. The authors found that ultrasound depicted breast masses associated with microcalcifications in approximately 45% of cases. Of these masses, 23% were benign and 82% were malignant.
The percentage of detection of masses was much higher if only clusters of malignant microcalcifications >10 mm were considered. Ultrasound masses associated with this subgroup were found in 100% of cases. Ultrasound can, therefore, be utilized in the visualization of masses associated with clusters of microcalcifications >10 mm that have a high suspicion of malignancy. The potential benefit is that it provides an alternative means of biopsy in patients who cannot undergo a stereotactic biopsy and do not desire excisional biopsy.
A pilot study performed by Soo et al 16 performed ultrasound-guided biopsy with 100% success in 23 patients with suspicious microcalcifications detected on mammography. The authors commented on the need for further study to determine whether sonographic targeting of microcalcifications might improve the rate of underestimation of disease when compared with stereotactic biopsy.
Conclusion
Ultrasound plays an essential role in the evaluation of the breast. It has progressed from its former limited role of determining whether a mass is cystic or solid into a method to assist in the differentiation of a benign from a malignant lesion. It is particularly useful in dense breast tissue. The ability to correlate a benign ultrasound mass with a mammographic mass eliminates the need for further intervention. Alternatively, the finding of a sonographically suspicious mass provides the necessary information for determining the need for histologic diagnosis. An added benefit is that the ultrasound-detected abnormality can be biopsied with ultrasound-guided core biopsy, thereby eliminating the need for excisional biopsy.