Radiological Case of the Month: Ureteropelvic junction
Prepared by Shawn Corey, MD, PhD, Robert Bechtold, MD, and Raymond Dyer, MD, Department of Radiology, Wake Forest Baptist Medical Center, Winston-Salem, NC.
CASE SUMMARY
A 30-year-old woman presented to her primary-care physician with a 2-year history of intermittent right flank pain. The pain typically occurred on weekends after episodes of binge drinking. A urine dipstick was negative for blood. Her creatinine level was 0.9 mg/dL, and her blood pressure was mildly elevated.
DIAGNOSIS
Ureteropelvic junction obstruction in the lower moiety of an incompletely duplicated collecting system secondary to an accessory precaval renal artery
IMAGING FINDINGS
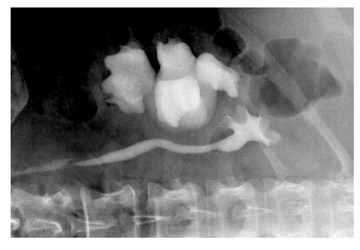
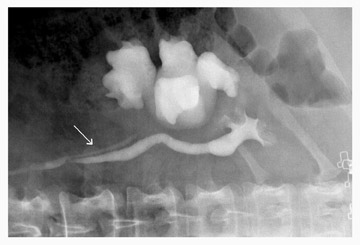
This patient's repeated episodes of right flank pain suggested partial obstruction of the right renal collecting system. Standard radiographs obtained after intravenous administration of contrast material for computed tomography (CT) revealed incomplete duplication of the right renal collecting system (Figure 1). The lower moiety collecting system was dilated, whereas the upper moiety collecting system was normal (Figure 1A). During fluoroscopy, arterial pulsations were observed at the ureteropelvic junction (UPJ) of the lower moiety, which suggested that a crossing vessel was contributing to the UPJ obstruction. In the supine position, little contrast material passed from the lower moiety collecting system into its ureter. Instead, contrast material refluxed from the shared right ureter into the lower moiety collecting system, indicative of yo-yo reflux (Figure 1B).
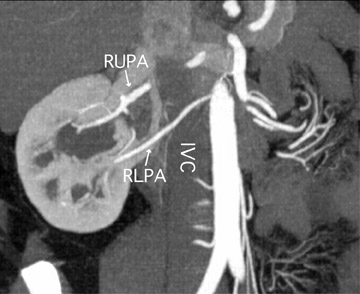
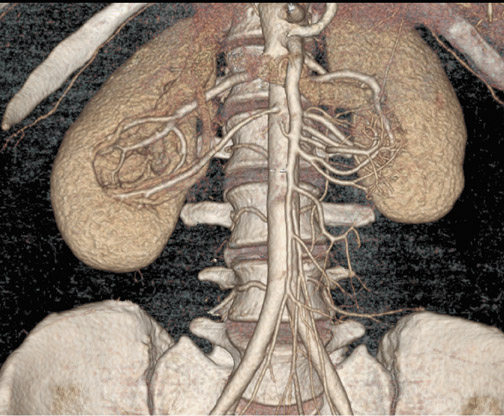
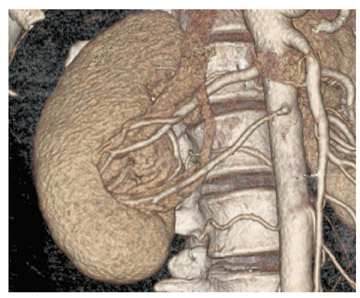
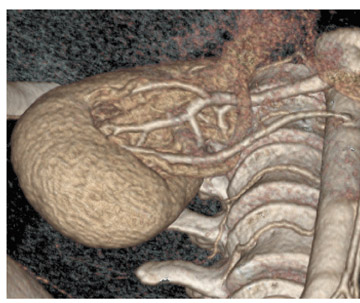
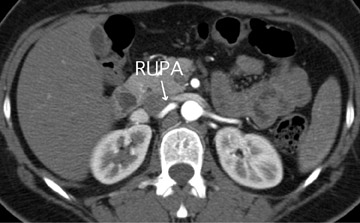
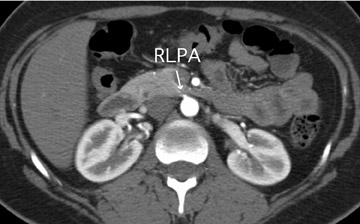
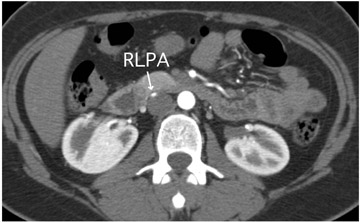
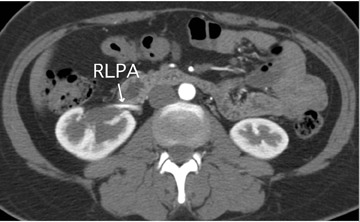
An oblique coronal CT reconstruction showed 2 right renal arteries (Figure 2A). The right upper pole artery (RUPA) crossed posterior to the inferior vena cava (IVC), whereas the right lower pole artery (RLPA) crossed anterior to the inferior vena cava (IVC). Three-dimensional (3D) volume-rendered images verified this finding and the spatial relationships (Figures 2B, C, and D). Axial imaging confirmed the location of the renal arteries relative to the IVC (Figure 3). The right lower pole renal artery and two renal veins crossed the UPJ at the site of obstruction (Figure 3D). This was also the site where vascular pulsations were noted at fluoroscopy. Surgical correction for partial UPJ obstruction secondary to a precaval right renal artery was recommended. Currently, the patient has opted for conservative management.
DISCUSSION
In adults, partial obstruction of a ureter or renal collecting system often presents as intermittent flank pain exacerbated by the consumption of large volumes of fluids. The condition that occurs with binge beer drinking, as was the case for this patient, has been coined "beer drinker's hydronephrosis." In children, typical symptoms of partial obstruction include pain, nausea, vomiting, hematuria after trauma, or an abdominal mass. 1 The exact incidence of UPJ obstruction in the setting of incomplete ureteral duplication is uncertain but is considered exceedingly rare. Obstruction in duplex systems was originally described at the lower pole UPJ; however, it is now known to occur at the upper pole UPJ as well. 2
Renal vascular variations are becoming increasingly easy to recognize with advances in CT and contrast-enhanced ultrasound. 3-6 Renal artery duplication occurs in approximately 25% of the population. On the other hand, precaval renal arteries are rare and occur in approximately 0.8% of the population. 7 Precaval renal arteries have been reported with normal renal position and rotation, fused enlarged kidneys, and bifid collecting systems. 8 The precaval artery often feeds the lower pole, has a similar caliber to the main renal artery, and is found dorsal to the gonadal vein. 8 Precaval renal arteries are important to recognize, because they can be mistaken for an aberrant hepatic artery during sonography and are relevant to surgical planning for nephrectomy and aortic replacement. 8
In approximately 50% of patients with UPJ obstruction, a crossing vessel plays a contributing role. 1,5 Both crossing arteries and veins can lead to obstruction. 5 CT is highly accurate both in detecting an obstruction and in determining whether there is an associated crossing ves-sel. 5
Correction of UPJ obstruction can be accomplished by either endourologic or surgical approaches. Endourologic approaches involve inserting a cutting device into the ureter across a stenotic segment. A vertical incision is made at the site of obstruction, which is then supported with a stent. In laproscopic or open surgical pyeloplasty, the renal pelvis and proximal ureter are surgically reconstructed. During the endourologic approach, failure to recognize a crossing vessel can lead to vascular injury. In addition, endopyelotomy success rates drop from 82% to 33% in the presence of a crossing vessel 9 (others report slightly better rates of 42% to 64% 10 ). On the other hand, laparoscopic pyeloplasty has been reported to be 86% to 100% successful in cases with a crossing vessel and seldom leads to vascular injury. 11 Thus, in the presence of a crossing vessel, a laparoscopic or open approach is preferred over endopyelotomy because of increased safety and efficacy. Many medical centers have deemed it worthwhile to adopt special imaging protocols in order to detect vascular variations prior to surgery. Often, these protocols include high-resolution CT followed by 3D volume rendering. 4,6
CONCLUSION
CT is highly accurate at depicting renovascular anatomy, detecting UPJ obstructions, and determining whether a crossing vessel is playing a contributing role. Recognition of crossing vessels prior to surgery can decrease the risk of vascular injury, improve surgical outcomes, and alter the surgical approach. Although precaval renal arteries occur rarely, they are important to recognize.