Isolated splenic metastasis in a patient with squamous cell carcinoma of the cervix
Images


CASE SUMMARY
Our patient is a 62-year-old Hispanic female with a past medical history of hypertension. She originally presented to the gynecologist with a chief complaint of post-menopausal bleeding. Physical examination and laboratory analysis were within normal limits. She underwent a hysteroscopy, dilation and curettage as well as a polypectomy. Pathology showed invasive squamous cell carcinoma of the cervix. A radical hysterectomy was then performed and surgical margins were negative. Adjunctive treatment with brachytherapy was conducted. The patient subsequently developed a ureteral stricture secondary to her radiation therapy, and follow-up imaging after ureteral stenting demonstrated a new hypodense lesion within the spleen.
IMAGING FINDINGS
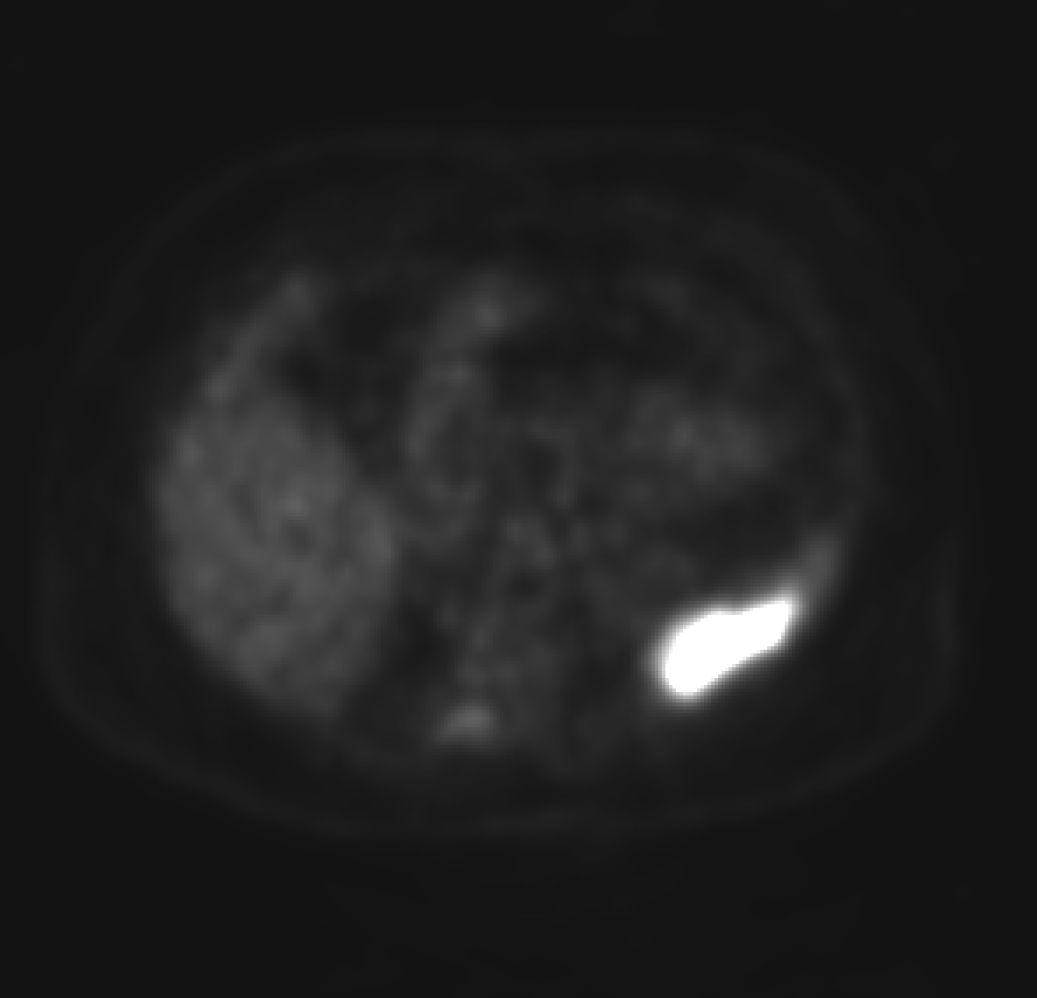
Computed tomographic image obtained during the portal venous phase demonstrates an ill-defined hypoattenuating lesion within the inferior portion of the spleen (Figure 1). Further imaging with positron emission tomography (Figures 2-3) showed the splenic lesion to be intensely FDG avid with a standardized uptake value of approximately 14.0.
A splenectomy was performed for the hypodense, intensely FDG avid splenic lesion.
DIAGNOSIS
Pathology confirmed the splenic lesion as a metastatic deposit from the patient’s squamous cell carcinoma of the cervix. The differential diagnosis for an entity with the aforementioned imaging findings include splenic metastasis, primary splenic malignancy and splenic abscess/infection.
DISCUSSION
nitially, the hypodense lesion within the spleen had the imaging characteristics of a splenic infarction. However, the lesion continued to grow and a PET/CT was performed. Due to the high level of concern for malignancy, the patient subsequently underwent a splenectomy for what was diagnosed as an isolated splenic metastasis from squamous cell carcinoma of the cervix. As of today she is disease free and no other sites of metastatic disease have been identified.
Splenic metastases may be solitary or multiple but tend to be solitary. Imaging characteristics of splenic metastases are variable, but typically reflect that of their primary tumor. They typically appear hypoechoic and contain regions of internal vascularity on ultrasound. With computed tomography, the lesions are usually hypoattenuating on pre-contrast images and demonstrate inhomogeneous enhancement after contrast administration. As for magnetic resonance imaging, the lesions routinely are isointense-hyperintense (if melanin or blood containing) on T1WI/T2WI sequences, hypointense on early post-contrast T1WI sequences and isointense on delayed post-contrast T1WI sequences.1
Available literature regarding splenic metastases from cervical carcinoma is scant. Most information available to date focuses on scattered case reports, as well as autopsy series from 20-80 years ago. The lack of information is thought to be due to selection bias and an overall decrease in the number of subjects undergoing autopsy.
A retrospective chart review of 29,364 patients with malignant tumors by Sauer et al, demonstrated 6,137 patients with metastatic disease of which, only 59 (0.02%) patients had proven splenic metastases, three of which had isolated splenic metastasis.2 A retrospective chart review of autopsies over a period of 20 years by Schӧn et al. found 1,898 patients with malignant tumors. Only 57 of the patients were found to have metastatic disease to the spleen.3 The occurrence of splenic metastases in malignancy is reported to vary from 0.6%-30%3,4 with the most common primary malignancies to metastasize to the spleen arising from breast cancer, lung cancer and melanoma.3,5 Carson et al, examined 2,200 patients with cervical cancer, of which only 15.3% had distant metastases. Only 22 cases of splenic metastases secondary to cervical cancer have been reported in the literature with a range of 3-6 cases of isolated splenic metastases reported.6,7
Splenic metastases from epithelial cancers are rare while splenic metastases from cervical carcinoma are exceptionally rare. It is theorized that cervical carcinoma metastases to the spleen are rare due to the main mechanism of spread via local invasion and lymphatics, rather than hematogenous spread.4 Historical theories regarding splenic metastases cite constant splenic blood flow, tortuosity of the splenic vessels, contractions of the spleen, lack of afferent lymphatic vessels, presence of a splenic capsule, anti-tumor antibodies, and the concentrated presence of phagocytes in the spleen as contributing factors to the rarity of splenic metastases.6,8 A current theory proposed by Peters states that normal granulocytes undergo age-related apoptosis ex vivo in a linear fashion and exponential apoptosis in vivo due to the varying times of granulocytes flowing through the spleen. This suggests a conversion from age-related, linear apoptosis to exponential, random apoptosis due to varying intersplenic exposure times of granulocytes to the pro-apoptotic environment of the spleen. Henceforth, tumor cells struggle to survive within the spleen.9
CONCLUSION
Hypodense lesions within the spleen should be approached with an appropriate level of clinical suspicion. The most common malignancies to metastasize to the spleen are lung cancer, breast cancer and melanoma. Splenic metastases from cervical carcinoma are rare while isolated splenic metastases from squamous cell carcinoma of the cervix are exceptionally rare.
REFERENCES
- Bowerson M, Menias C, Lee K, Fowler K, et al. Hot spleen: hypervascular lesions of the spleen. Abdominal Imaging. 2015;40(7):2796-2813.
- Sauer J, et al. Splenic metastases − Not a frequent problem, but an underestimate location of metastases: epidemiology and course. Journal of Cancer Research and Clinical Oncology. 2008;135(5):667-671.
- Schön CA, et al. Splenic metastases in a large unselected autopsy series. Pathology - Research and Practice. 2006;202(5):351-356.
- Taga Shigeki S. Splenic metastasis of squamous cell carcinoma of the uterine cervix: a case report and review of the literature. Case Reports in Obstetrics Gynecology. 2014.
- Klein BB. Splenomegaly and solitary spleen metastasis in solid tumors. Cancer. 1987;60(1):100-102.
- Gupta TT. Splenic metastases from cervical carcinoma: a case report. International Journal of Gynecological Cancer. 2006;16(2):911-914.
- Aitelhaj Meryem M. Breast and splenic metastases of squamous cell carcinoma from the uterine cervix: a case report. Journal of Medical Case Reports. 2014;8.
- Piura B, Rabinovich A, Apel-Sarid L, Shaco-Levy R. Splenic metastasis from endometrial carcinoma: report of a case and review of literature. Archives of Gynecology and Obstetrics. 2009;280(6):1001-1006.
- Peters AM. Why the spleen is a very rare site for metastases from epithelial cancers. Medical Hypotheses. 2011;78(1):26-28.
Citation
M A, B S. Isolated splenic metastasis in a patient with squamous cell carcinoma of the cervix. Appl Radiol. 2017;(6):24-25.
June 8, 2017