Intracardiac cement embolus from vertebroplasty
Images


CASE SUMMARY
A 72-year-old female initially presented to the emergency department with severe low back pain after using her bedside commode at home. Radiographs of the lumbar spine showed age-indeterminate compression deformities of the L1 and L2 vertebral bodies. Subsequent magnetic resonance imaging (MRI) confirmed acuity of the fractures. The patient underwent percutaneous vertebroplasty with polymethyl methacrylate of both L1 and L2, and was later discharged.
The patient was readmitted seven months later, following a fall. Abdominal radiograph showed a nonspecific linear density projecting over the spine (Figure 1). Computed tomography (CT) of the abdomen and pelvis was then performed, and demonstrated a high-attenuation linear structure extending from the mid inferior vena cava (IVC) into the right ventricle (Figure 2). Initially, the finding was thought to represent an abandoned catheter.
IMAGING FINDINGS
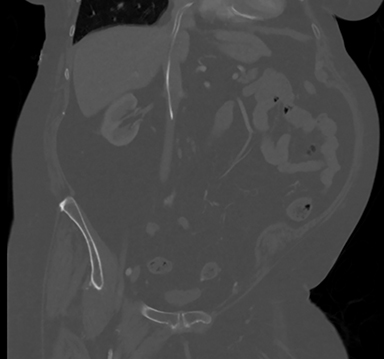
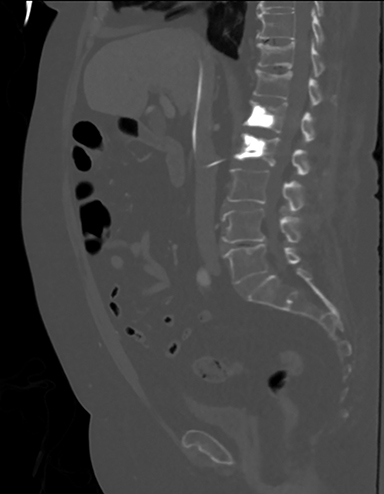
Upon review of perioperative fluoroscopic images from the patient’s vertebroplasty (not shown), the foreign body was absent prior to, and present after injection of cement material. Closer scrutiny of the CT showed cement extending from a paravertebral vein at the L2 vertebral body into the IVC (Figures 3 and 4), and into the right atrium and ventricle.
DIAGNOSIS
Cement embolus from vertebroplasty
DISCUSSION
Vertebroplasty procedures aim to reduce pain, height loss and kyphosis from vertebral body compression fractures. Vertebroplasty is superior to medical management, especially with regards to overall quality of life.1. Major complications of vertebroplasty are rare, although not unheard of. The most frequent and potentially serious complications are related to cement leakage. Common locations of cement extravasation include the intervertebral disc space, epidural space and pulmonary arteries. In one study, cement leakage into the venous system was reported in nearly a quarter of cases of pulmonary cement emboli seen on chest radiograph, which occurred in 4.6% of cases of vertebroplasty and kyphoplasty.2 Fortunately, a very small percentage of patients experience symptoms from cement leakage.
A meta-analysis performed by Taylor et al. concluded that 81 out of 1,000 vertebroplasty procedures were complicated by a cement leakage, with only 0.9 out of 1,000 patients who underwent vertebroplasty procedures being symptomatic due to cement leakage.1 In some cases, cement leakage can be serious, despite being asymptomatic. A small number of case reports have described previously asymptomatic patients presenting emergently with right ventricular perforation from cement emboli.3,4
In the case of our patient, interventional radiology and cardiothoracic surgery were consulted for retrieval of the cement embolus. Both services believed that the risk of retrieval was greater than the potential complications that may arise from allowing the cement material to remain in situ, especially in light of the patient’s significant comorbidities. One year following identification of the cement embolus, the patient remains asymptomatic.
This case brings to light an important consideration in vertebroplasty-related cement leakage, which is that indications for cement retrieval are poorly defined in the literature. Although our patient has made it almost two years without major complications from her vertebroplasty and resulting cement embolus, there are documented cases where lack of identification and/or intervention resulted in right ventricular wall perforation, requiring emergent surgical removal and repair.3,4
CONCLUSION
Cement leakage is a rare but important potential complication of vertebroplasty. Many cases are undiagnosed at the time of the procedure, and are often discovered as incidental findings on future imaging. Although most patients remain asymptomatic, based on the location of the cement embolus, major complications may arise, including perforation of the cardiac wall.
REFERENCES
- Taylor RS, Fritzell P, Taylor RJ. Balloon kyphoplasty in the management of vertebral compression fractures: An updated systematic review and meta-analysis. Eur Spine J. 2007;16:1085-1100.
- Choe DH, Marom EM, Ahrar K, Troung MT, Madewell JE. Pulmonary embolism of polymethyl methacrylate during percutaneous vertebroplasty and kyphoplasty. AJR Am J Roentgenol. 2004;183:1097-1102.
- Ishikawa K, Hayashi H, Mori H. Cardiac perforation caused by cement after percutaneous balloon kyphoplasty. Asian Cardiovasc Thorac Ann. 2015;23(9):1-3.
- Gosev I, Nascimben L, Huang PH, Mauri L, Steigner M, Mizuguchi A, Shah A, Aranki S. Right ventricular perforation and pulmonary embolism with polymethyl methacrylate cement after percutaneous kyphoplasty. Circulation. 2013;127:1251-1253.
Citation
H H, AJ L, M M, G G. Intracardiac cement embolus from vertebroplasty. Appl Radiol. 2017;(1):47C-47D.
January 10, 2017