Interventional Radiology: Inferior vena cava filters—Update on placement and retrieval
Images




Pulmonary embolism (PE) is a leading cause of morbidity and mortality in the United States, causing 50,000 to 200,000 deaths yearly.1 While anticoagulation is the gold standard of treatment, interruption of the inferior vena cava (IVC) is indicated in those whom anticoagulation is contraindicated or has failed. The role of IVC filter placement is only to prevent clinically significant PE by trapping venous emboli.2 Recurrent PE following filter placement is very low, reported as approximately 2%-5% of cases.3
Currently, the indications for IVC filter placement are therapeutic and prophylactic. Therapeutic indications are those that have documented venous thromboembolism (VTE) and at least one of the following: absolute or relative contraindications to anticoagulation, complications from prior anticoagulation, failure of anticoagulation, recurrent PE despite anticoagulation, progression of deep venous thrombosis (DVT) while on anticoagulation, massive PE with residual DVT in a patient at risk for additional PE, free-floating iliofemoral or IVC thrombus, and DVT with severe cardiopulmonary disease.1 Prophylactic indications include severe trauma, closed head injury, spinal cord injury, multiple long-bone or pelvic fractures, and immobilized patients at high risk. The only absolute contraindications to filter placement are not having an access route to the vena cava and not having a large enough location within the vena cava for placement.2 Relative contraindications include severe coagulopathy and bacteremia.1
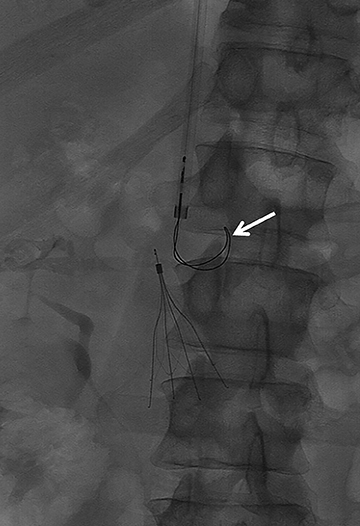
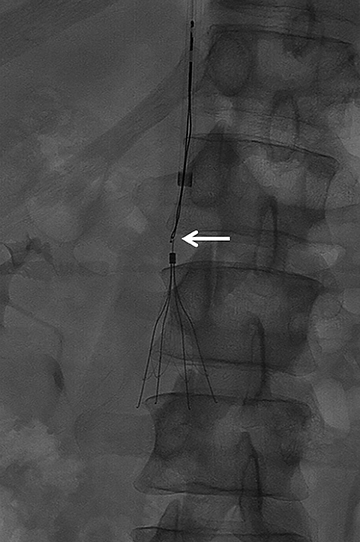
The majority of IVC filters are placed within the infrarenal IVC; however, there are few indications for placement in the suprarenal IVC, such as pregnancy and gonadal vein thrombosis. Filters can be permanent or retrievable, and permanent filters have been placed since the 1970s with few complications. Retrievable filters are placed for the same indications as permanent filters; however, they are used when the need for filtration protection against PE is anticipated to be short. Removing the filter is an option when an indication for an IVC filter is no longer present, the risk of clinically significant PE is acceptably low as a result of the primary therapy, the patient is not anticipated to return to a high risk for PE, the patient’s life expectancy is long enough that the patient will benefit from filter removal, and the filter can be safely removed.2 (Figures 1 and 2).
Traditionally, time limits are in place for filter retrieval. More recently, data suggests very high success rates of >60% when Gunther Tulip filters (Cook Medical: Bloomington, Indiana) were removed up to 17 months after insertion.4 However, several case reports state that different brands of filters were removed after extended periods, well beyond manufacturers’ recommendations.5
With the emergence of prophylactic filter indications, the number of retrievable filters placed has increased. On retrieval, a vena cavagram must be performed to evaluate for clot burden within the filter. If >25% of the filter’s cone volume contains a clot, the filter should not be removed.6 Many retrievable filters are not removed in a timely manner (based on the manufacturers’ recommendations). This is most commonly due to lack of appropriate follow-up with interventional radiology. By instituting an IVC filter clinic, Gupta and his colleagues reported an increase in retrieval rates, from 29%-62%.7 Other inhibitions to filter removal may be tilting of the filter after placement or penetration of a filter strut. Yoon and his coworkers studied Cook, Bard (Tempe, Arizona), ALN (Miami, Florida) and Cordis (Bridgewater, New Jersey) filters that were placed in their institution from 2007 to 2010. They found that all filter brands demonstrated changes in their angle, migrated minimally and penetrated the IVC wall.8 However, the recent trial involving Bard’s Denali Filter outlines improved success rates in retrieving this filter due to lower rates of tilt, fracture and migration.9
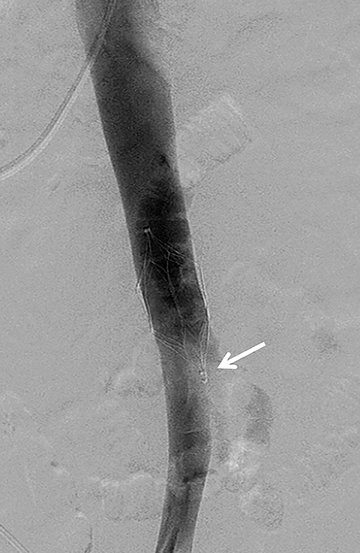
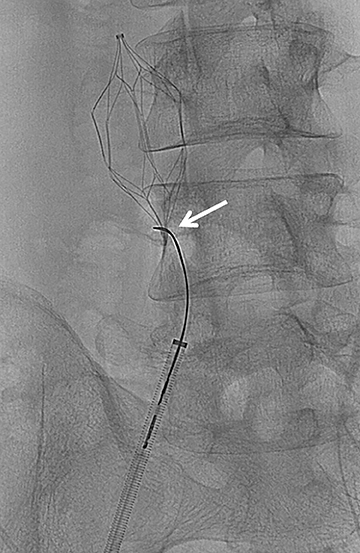
A devastating complication of filter placement is caval thrombosis, especially when filters are placed for prophylaxis. This may warrant additional imaging surveillance, further intervention and a hospital stay.10 In a series by Corriere and his colleagues, IVC thrombosis was seen in 12% of the cases with retrievable filters, and 6% with permanent filters.10 Thrombosis of the access site may also occur, and ranges from 2%-25%, the range being altered by the type of delivery system.3 As many as 30%-35% of patients may experience clinical signs of venous insufficiency at 6 years even when treated with anticoagulation following filter placement. Other complications from filter placement include filter fracture (1%), filter migration (3%-69%), and penetration of the IVC (9%-24%)3 (Figures 3 and 4). Therefore, it is imperative that the patient have a true, realistic and solid indication for IVC filter placement that is supported by documented clinical evidence.
While anticoagulation remains the overall gold standard in treating venous thromboembolism, IVC filters are a safe and effective means of PE prevention, and warrant consideration in patients who have a contraindication, failure or complication from anticoagulation.
REFERENCES
- Caplin DM, Nikolic B, Kalva SP, et al. Quality improvement guidelines for the performance of inferior vena cava filter placement for the prevention of pulmonary embolism. J Vasc Interv Radiol. 2011;22:1499-1506.
- Kaufman JA, Kinney TB, Streiff MB, et al. Guidelines for the use of retrievable and convertible vena cava filters: Report from the Society of Interventional Radiology Multidisciplinary Consensus Conference. J Vasc Interv Radiol. 2006;17:449-459.
- Kinney TB. Update on inferior vena cava filters. J Vasc Interv Radiol. 2003;14:425-440.
- Smouse HB, Rosenthal D, Thuong VH, et al. Long-term retrieval success rate profile for the Günther Tulip vena cava filter. J Vasc Interv Radiol. 2009;20(7):871-877.
- Lynch FC. Removal of a Gunther Tulip filter after 3,006 days. J Vasc Interv Radiol. 2011;22:337-340.
- Dinglasan LV, Stavropoulos SW, Shlansky-Goldberg R, et al. Removal of fractured retrievable IVC filters: Feasibility and outcomes. J Vasc Interv Radiol. 2011, S47.
- Gupta R, Minocha J, Riaz A, et al. Optimizing IVC filter utilization: The impact of a dedicated IVC filter clinic. J Vasc Interv Radiol. 2011;22(3),S45.
- Yoon JP, Valenti DA, Cabrera T, et al. Changes in tilt angle, position and penetration of inferior vena cava (IVC) wall of ALN, Bard, Cook and Cordis retrievable IVC filters. J Vasc Interv Radiol. 2011,22(3),S144.
- Stavropoulos SW, Sing RF, Elmasri F, et al. The DENALI Trial: An interim analysis of a prospective, multicenter study of the Denali Retrievable Inferior Vena Cava Filter. J Vasc Interv Radiol. July 24, 2014;S1051-0443(14)00653-8. [Epub ahead of print].
- Corriere MA, Suave KJ, Ayerdi J, et al. Vena cava filters and inferior vena cava thrombosis. J Vasc Surg. 2007;45(4):789-794.